

The importance of taking ART appropriately in children and adolescents with HIV-1 to reach the highest capacity of immune function later in life
- PMID: 35967315
- PMCID: PMC9364750
- DOI: 10.3389/fimmu.2022.860316
The importance of taking ART appropriately in children and adolescents with HIV-1 to reach the highest capacity of immune function later in life
Abstract
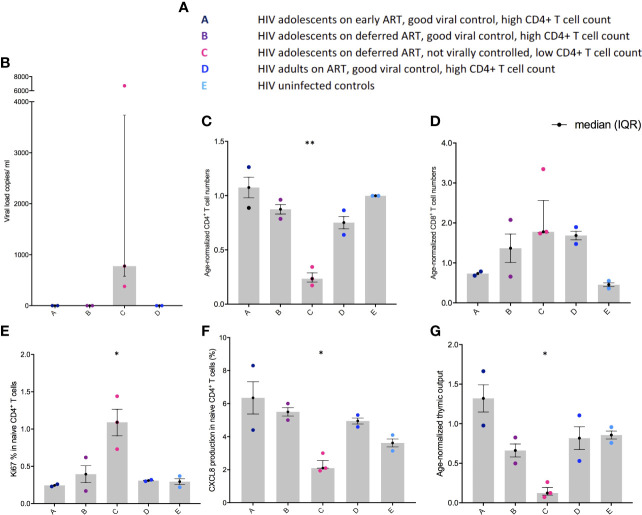
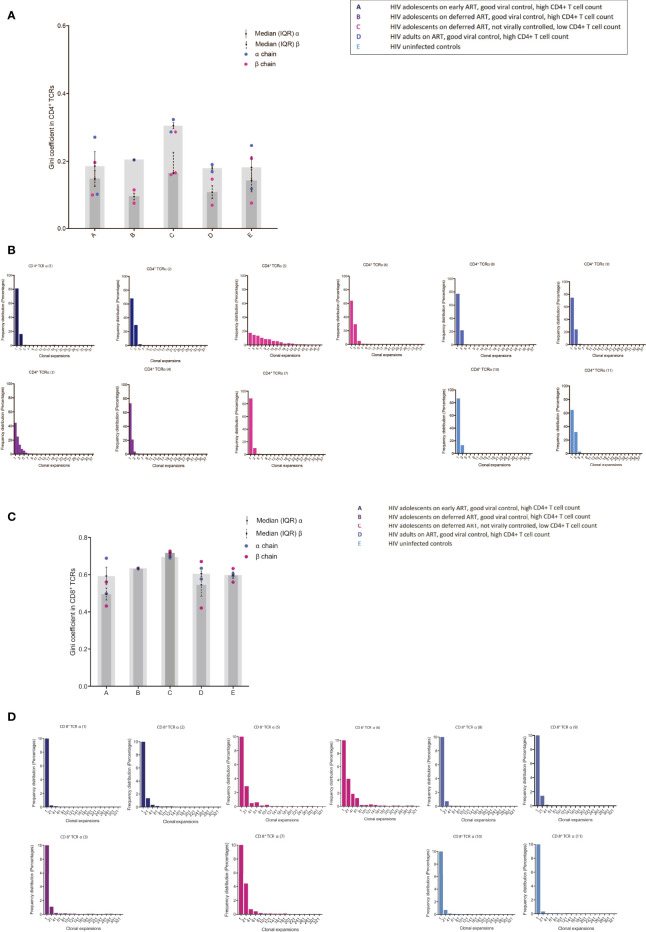
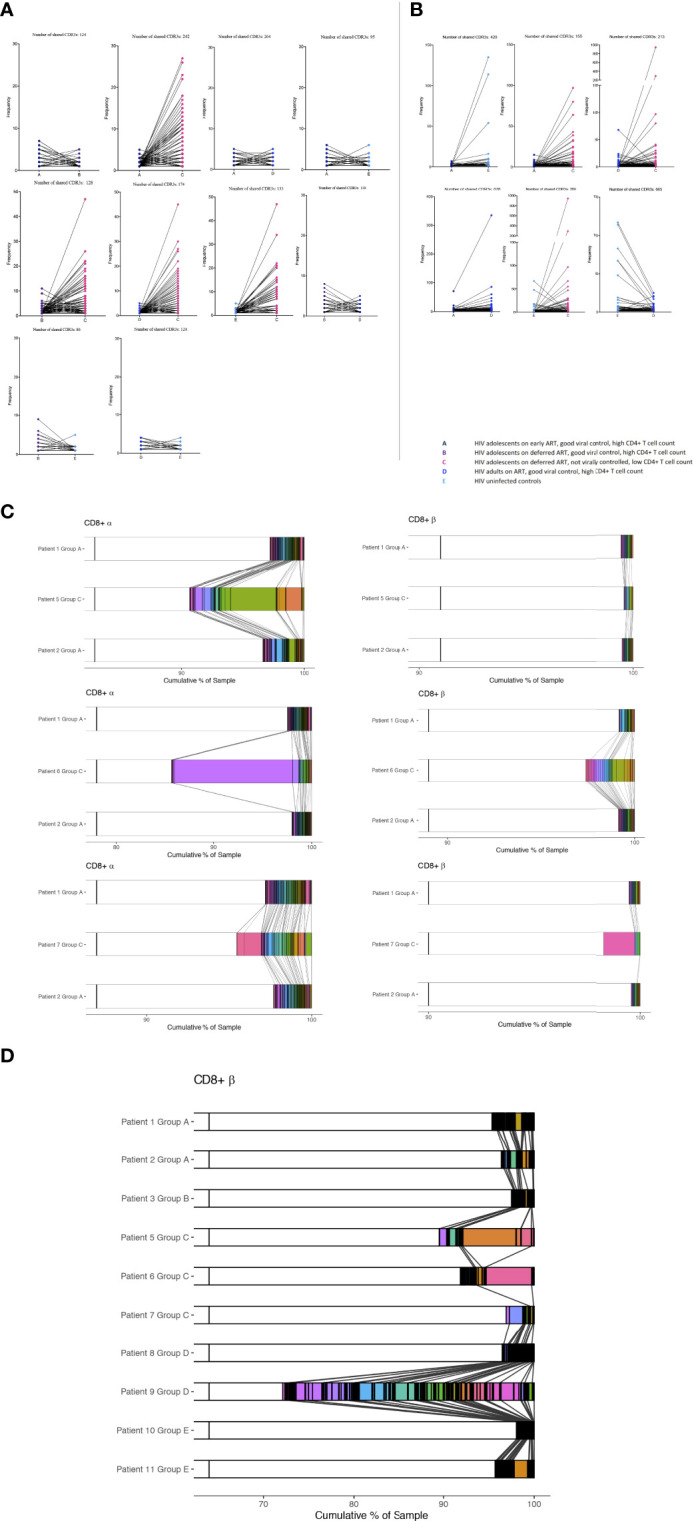
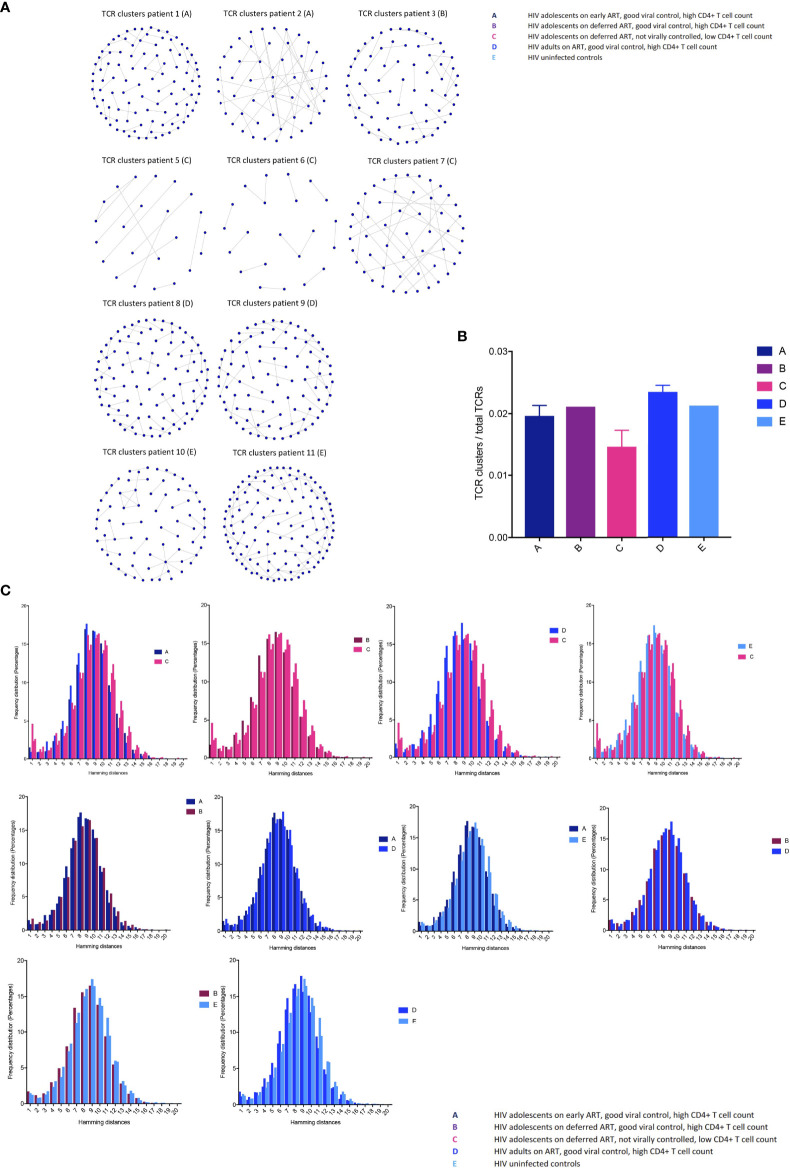
Current antiretroviral therapy (ART) guidelines recommend treating all children with HIV-1 infection. This has changed from the broader use of ART to treat children to improve morbidity and minimise mortality. However, prior to current recommendations, not everyone with HIV-1 received timely treatment. What happens to the paediatric immune system when HIV-1 replication is not appropriately supressed remains unclear. 11 samples from adolescents with HIV-1 on ART and uninfected controls in the UK, aged 12-25 years, were examined; overall, adolescents with CD4+ counts > 500/μl and a viral load < 50 copies/ml were compared with adolescents with CD4+ counts < 500/μl and a viral load > 50 copies/ml at time of sampling. Measurements of thymic output were combined with high throughput next generation sequencing and bioinformatics to systematically organize CD4+ and CD8+ T cell receptor (TCR) repertoires. TCR repertoire diversity, clonal expansions, TCR sequence sharing, and formation of TCR clusters in HIV-1 infected adolescents with successful HIV-1 suppression were compared to adolescents with ineffective HIV-1 suppression. Thymic output and CD4+ T cell numbers were decreased in HIV-1 infected adolescents with poor HIV-1 suppression. A strong homeostatic TCR response, driven by the decreased CD4+ T cell compartment and reduced thymic output was observed in the virally uncontrolled HIV-1-infected adolescents. Formation of abundant robust TCR clusters and structurally related TCRs were found in the adolescents with effective HIV-1 suppression. Numerous CD4+ T cell numbers in the virally controlled adolescents emphasize the importance of high thymic output and formation of robust TCR clusters in the maintenance of HIV-1 suppression. While the profound capacity for immune recovery in children may allow better opportunity to deal with immunological stress, when ART is taken appropriately, this study demonstrates new insights into the unique paediatric immune system and the immunological changes when HIV-1 replication is ongoing.
Keywords: HIV-1; T cell receptor clonal expansions; T cell receptor repertoires; antiretroviral therapy (ART); children; high throughout sequencing; immune reconstitution; thymic output.
Copyright © 2022 Sandgaard, Gkouleli, Attenborough, Adams, Gibbons, Holm, Eisen, Baxendale, De Rossi, Pahwa, Chain, Gkazi and Klein.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Plasticity of the Immune System in Children Following Treatment Interruption in HIV-1 Infection.Front Immunol. 2021 Jul 29;12:643189. doi: 10.3389/fimmu.2021.643189. eCollection 2021. Front Immunol. 2021. PMID: 34475868 Free PMC article. Clinical Trial.
-
Antiretroviral therapy restores diversity in the T-cell receptor Vbeta repertoire of CD4 T-cell subpopulations among human immunodeficiency virus type 1-infected children and adolescents.Clin Vaccine Immunol. 2009 Sep;16(9):1293-301. doi: 10.1128/CVI.00074-09. Epub 2009 Jul 15. Clin Vaccine Immunol. 2009. PMID: 19605599 Free PMC article.
-
Thymic function in HIV-infection.Dan Med J. 2013 Apr;60(4):B4622. Dan Med J. 2013. PMID: 23651726 Review.
-
The pattern and magnitude of T cell subsets reconstitution during ten years of ART with viral suppression in HIV-infected patients.Aging (Albany NY). 2022 Dec 9;14(23):9647-9667. doi: 10.18632/aging.204416. Epub 2022 Dec 9. Aging (Albany NY). 2022. PMID: 36490352 Free PMC article.
-
Multi-omics in HIV: searching insights to understand immunological non-response in PLHIV.Front Immunol. 2023 Aug 15;14:1228795. doi: 10.3389/fimmu.2023.1228795. eCollection 2023. Front Immunol. 2023. PMID: 37649488 Free PMC article. Review.
Cited by
-
Evolution of CD4 T-Cell Count With Age in a Cohort of Young People Growing Up With Perinatally Acquired Human Immunodeficiency Virus.Clin Infect Dis. 2024 Mar 20;78(3):690-701. doi: 10.1093/cid/ciad626. Clin Infect Dis. 2024. PMID: 37820036 Free PMC article.
-
Analysis of the clinical characteristics of poor immunological reconstitution in AIDS patients after long-term antiviral therapy in Xinjiang, China.BMC Immunol. 2025 Jul 4;26(1):48. doi: 10.1186/s12865-025-00732-5. BMC Immunol. 2025. PMID: 40615782 Free PMC article.
References
-
- Cotton MF, Violari A, Otwombe K, Panchia R, Dobbels E, Rabie H, et al. . Early time-limited antiretroviral therapy versus deferred therapy in south African infants infected with HIV: Results from the children with HIV early antiretroviral (CHER) randomised trial. Lancet (2013) 382(9904):1555–63. doi: 10.1016/S0140-6736(13)61409-9 - DOI - PMC - PubMed
-
- Bamford A, Turkova A, Lyall H, Foster C, Klein N, Bastiaans D, et al. . Paediatric European network for treatment of AIDS (PENTA) guidelines for treatment of paediatric HIV-1 infection 2015: Optimizing health in preparation for adult life. HIV Med (2018) 19(1):e1–e42. doi: 10.1111/hiv.12217 - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials