

Multiplex protein profiling of bronchial aspirates reveals disease-, mortality- and respiratory sequelae-associated signatures in critically ill patients with ARDS secondary to SARS-CoV-2 infection
- PMID: 35967328
- PMCID: PMC9373836
- DOI: 10.3389/fimmu.2022.942443
Multiplex protein profiling of bronchial aspirates reveals disease-, mortality- and respiratory sequelae-associated signatures in critically ill patients with ARDS secondary to SARS-CoV-2 infection
Abstract
Introduction: Bronchial aspirates (BAS) obtained during invasive mechanical ventilation (IMV) constitutes a useful tool for molecular phenotyping and decision making.
Aim: To identify the proteomic determinants associated with disease pathogenesis, all-cause mortality and respiratory sequelae in BAS samples from critically ill patients with SARS-CoV-2-induced ARDS.
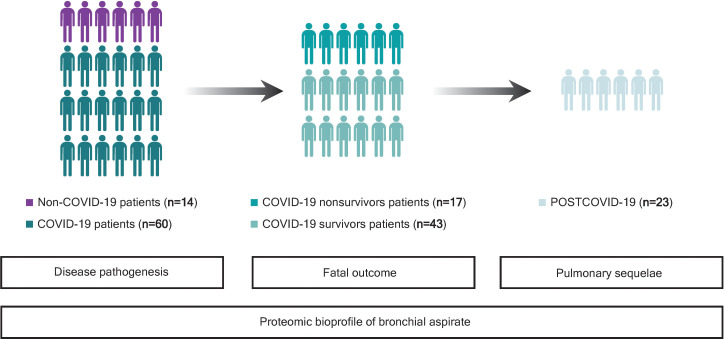
Methods: Multicenter study including 74 critically ill patients with COVID-19 and non-COVID-19 ARDS. BAS were obtained by bronchoaspiration after IMV initiation. Three hundred sixty-four proteins were quantified using proximity extension assay (PEA) technology. Random forest models were used to assess predictor importance.
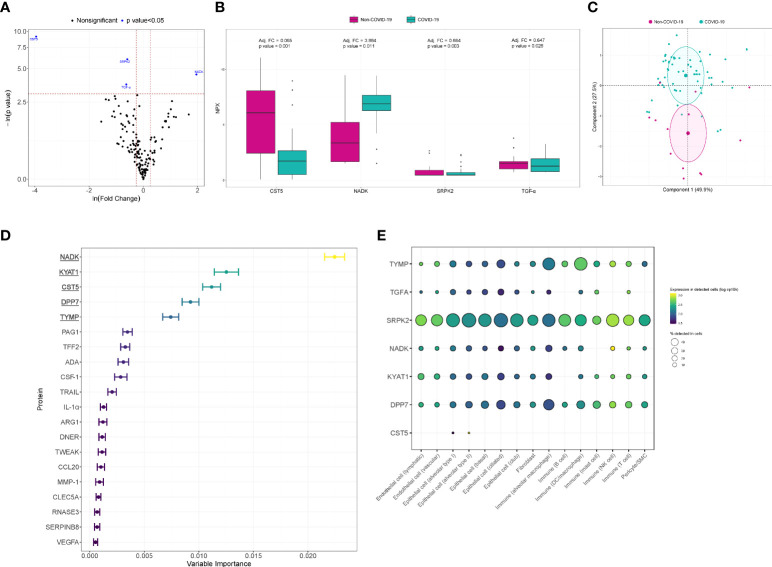
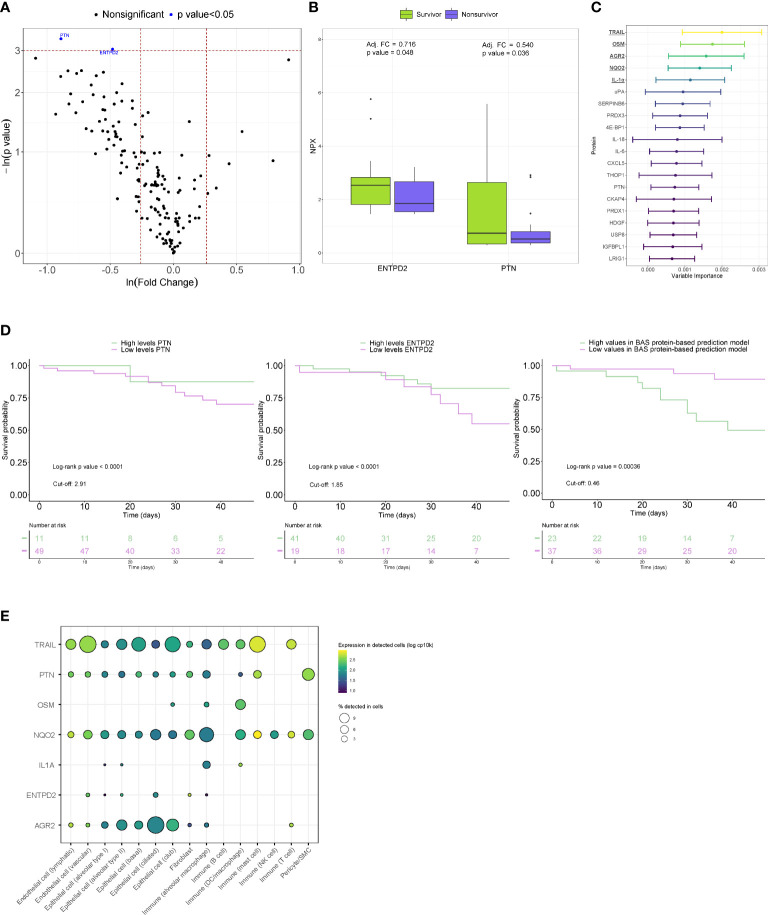
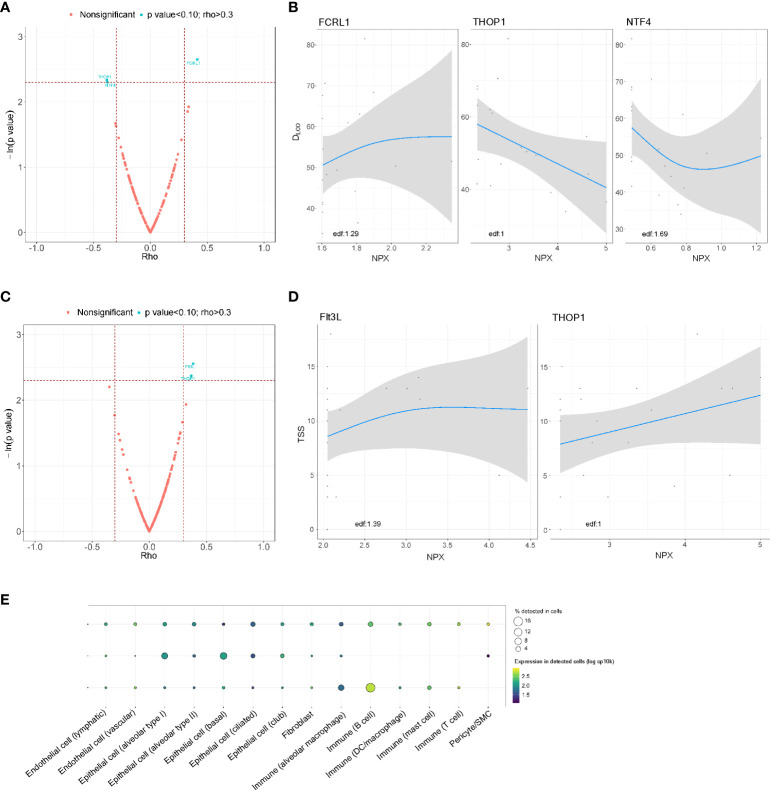
Results: After adjusting for confounding factors, CST5, NADK, SRPK2 and TGF-α were differentially detected in COVID-19 and non-COVID-19 patients. In random forest models for COVID-19, CST5, DPP7, NADK, KYAT1 and TYMP showed the highest variable importance. In COVID-19 patients, reduced levels of ENTPD2 and PTN were observed in nonsurvivors of ICU stay, even after adjustment. AGR2, NQO2, IL-1α, OSM and TRAIL showed the strongest associations with in-ICU mortality and were used to construct a protein-based prediction model. Kaplan-Meier curves revealed a clear separation in mortality risk between subgroups of PTN, ENTPD2 and the prediction model. Cox regression models supported these findings. In survivors, the levels of FCRL1, NTF4 and THOP1 in BAS samples obtained during the ICU stay correlated with lung function (i.e., DLCO levels) 3 months after hospital discharge. Similarly, Flt3L and THOP1 levels were correlated with radiological features (i.e., TSS). These proteins are expressed in immune and nonimmune lung cells. Poor host response to viral infectivity and an inappropriate reparative mechanism seem to be linked with the pathogenesis of the disease and fatal outcomes, respectively.
Conclusion: BAS proteomics identified novel factors associated with the pathology of SARS-CoV-2-induced ARDS and its adverse outcomes. BAS-based protein testing emerges as a novel tool for risk assessment in the ICU.
Keywords: COVID-19; ICU – intensive care unit; acute respiratory distress syndrome; bronchial aspirate; proteomics.
Copyright © 2022 Molinero, Gómez, Benítez, Vengoechea, González, Polanco, Gort-Paniello, Moncusí-Moix, García-Hidalgo, Perez-Pons, Belmonte, Torres, Caballero, Barberà, Ayestarán Rota, Socías Crespí, Ceccato, Fernández-Barat, Ferrer, Garcia-Gasulla, Lorente-Balanza, Menéndez, Motos, Peñuelas, Riera, Torres, Barbé and de Gonzalo-Calvo.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Bronchial Aspirate-Based Profiling Identifies MicroRNA Signatures Associated With COVID-19 and Fatal Disease in Critically Ill Patients.Front Med (Lausanne). 2022 Feb 3;8:756517. doi: 10.3389/fmed.2021.756517. eCollection 2021. Front Med (Lausanne). 2022. PMID: 35186962 Free PMC article.
-
Clinical characteristics and day-90 outcomes of 4244 critically ill adults with COVID-19: a prospective cohort study.Intensive Care Med. 2021 Jan;47(1):60-73. doi: 10.1007/s00134-020-06294-x. Epub 2020 Oct 29. Intensive Care Med. 2021. PMID: 33211135 Free PMC article.
-
Transpulmonary Plasma Endothelin-1 Arterial:Venous Ratio Differentiates Survivors from Non-Survivors in Critically Ill Patients with COVID-19-Induced Acute Respiratory Distress Syndrome.Int J Mol Sci. 2024 Oct 2;25(19):10640. doi: 10.3390/ijms251910640. Int J Mol Sci. 2024. PMID: 39408968 Free PMC article.
-
Outcomes of critically ill COVID-19 survivors and caregivers: a case study-centred narrative review.Can J Anaesth. 2022 May;69(5):630-643. doi: 10.1007/s12630-022-02194-4. Epub 2022 Jan 31. Can J Anaesth. 2022. PMID: 35102495 Free PMC article. Review.
-
Disruption of CCR5 signaling to treat COVID-19-associated cytokine storm: Case series of four critically ill patients treated with leronlimab.J Transl Autoimmun. 2021;4:100083. doi: 10.1016/j.jtauto.2021.100083. Epub 2021 Jan 6. J Transl Autoimmun. 2021. PMID: 33521616 Free PMC article. Review.
Cited by
-
Virus-Host Protein Interaction Network of the Hepatitis E Virus ORF2-4 by Mammalian Two-Hybrid Assays.Viruses. 2023 Dec 12;15(12):2412. doi: 10.3390/v15122412. Viruses. 2023. PMID: 38140653 Free PMC article.
-
Serine-arginine protein kinases and their targets in viral infection and their inhibition.Cell Mol Life Sci. 2023 May 17;80(6):153. doi: 10.1007/s00018-023-04808-6. Cell Mol Life Sci. 2023. PMID: 37198350 Free PMC article. Review.
-
Compartmentalization of the inflammatory response during bacterial sepsis and severe COVID-19.J Intensive Med. 2024 Feb 27;4(3):326-340. doi: 10.1016/j.jointm.2024.01.001. eCollection 2024 Jul. J Intensive Med. 2024. PMID: 39035623 Free PMC article. Review.
-
A Sequent of Gram-Negative Co-Infectome-Induced Acute Respiratory Distress Syndrome Are Potentially Subtle Aggravators Associated to the SARS-CoV-2 Evolution of Virulence.Diagnostics (Basel). 2024 Jan 4;14(1):120. doi: 10.3390/diagnostics14010120. Diagnostics (Basel). 2024. PMID: 38201429 Free PMC article.
-
Potential Immune-Inflammatory Proteome Biomarkers for Guiding the Treatment of Patients with Primary Acute Angle-Closure Glaucoma Caused by COVID-19.J Proteome Res. 2024 Jul 5;23(7):2587-2597. doi: 10.1021/acs.jproteome.4c00325. Epub 2024 Jun 5. J Proteome Res. 2024. PMID: 38836775 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous