

Classification of colon adenocarcinoma based on immunological characterizations: Implications for prognosis and immunotherapy
- PMID: 35967414
- PMCID: PMC9363576
- DOI: 10.3389/fimmu.2022.934083
Classification of colon adenocarcinoma based on immunological characterizations: Implications for prognosis and immunotherapy
Abstract
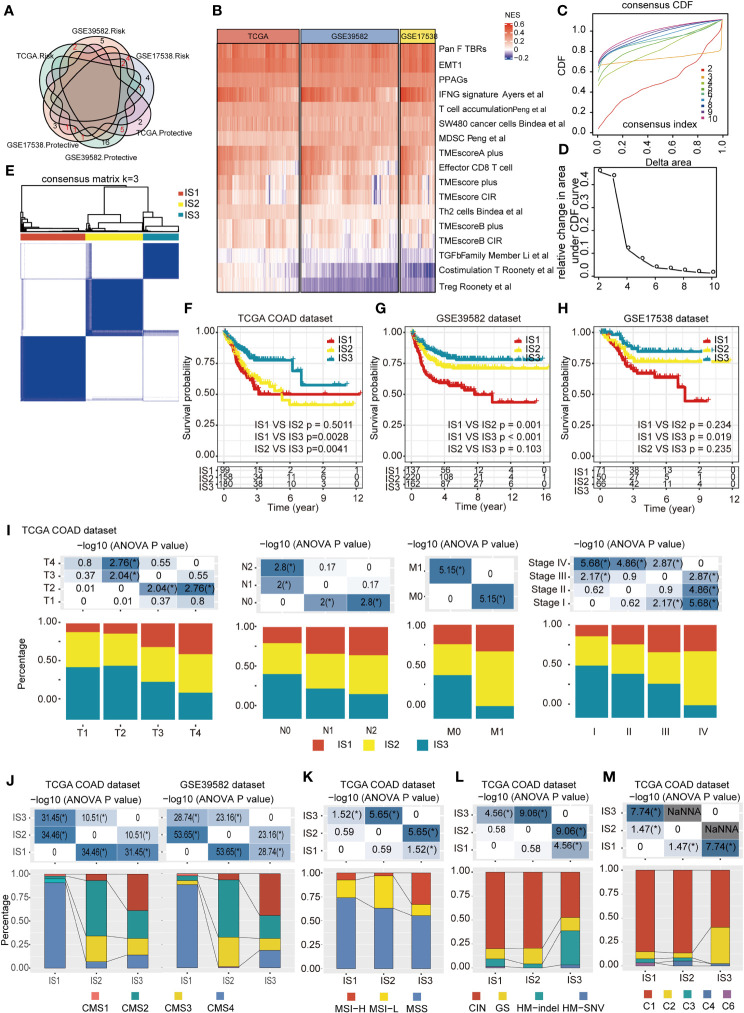
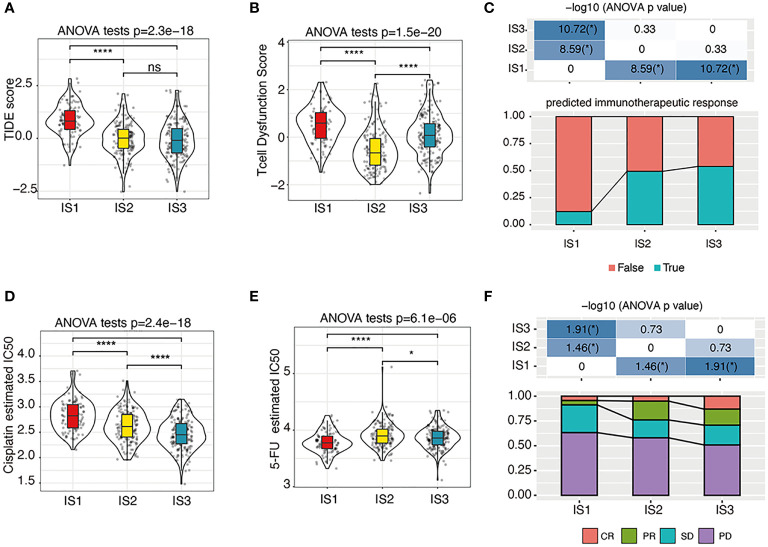
Accurate immune molecular typing is pivotal for screening out patients with colon adenocarcinoma (COAD) who may benefit from immunotherapy and whose tumor microenvironment (TME) was needed for reprogramming to beneficial immune-mediated responses. However, little is known about the immune characteristic of COAD. Here, by calculating the enrichment score of immune characteristics in three online COAD datasets (TCGA-COAD, GSE39582, and GSE17538), we identified 17 prognostic-related immune characteristics that overlapped in at least two datasets. We determined that COADs could be stratified into three immune subtypes (IS1-IS3), based on consensus clustering of these 17 immune characteristics. Each of the three ISs was associated with distinct clinicopathological characteristics, genetic aberrations, tumor-infiltrating immune cell composition, immunophenotyping (immune "hot" and immune "cold"), and cytokine profiles, as well as different clinical outcomes and immunotherapy/therapeutic response. Patients with the IS1 tumor had high immune infiltration but immunosuppressive phenotype, IS3 tumor is an immune "hot" phenotype, whereas those with the IS2 tumor had an immune "cold" phenotype. We further verified the distinct immune phenotype of IS1 and IS3 by an in-house COAD cohort. We propose that the immune subtyping can be utilized to identify COAD patients who will be affected by the tumor immune microenvironment. Furthermore, the ISs may provide a guide for personalized cancer immunotherapy and for tumor prognosis.
Keywords: colon adenocarcinoma; immune characteristics; immune subtype analysis; prognosis; therapy response.
Copyright © 2022 Xu, Chang, Wang, Wang, Wang, Weng, Tan, Zhang, Ni, Wang, Huang, Deng, Li, Huang and Sheng.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures





References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources