

Current status of xenotransplantation research and the strategies for preventing xenograft rejection
- PMID: 35967435
- PMCID: PMC9367636
- DOI: 10.3389/fimmu.2022.928173
Current status of xenotransplantation research and the strategies for preventing xenograft rejection
Abstract
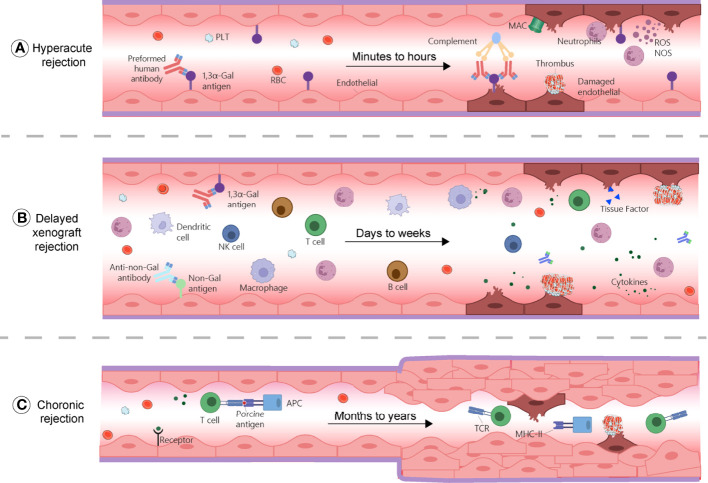
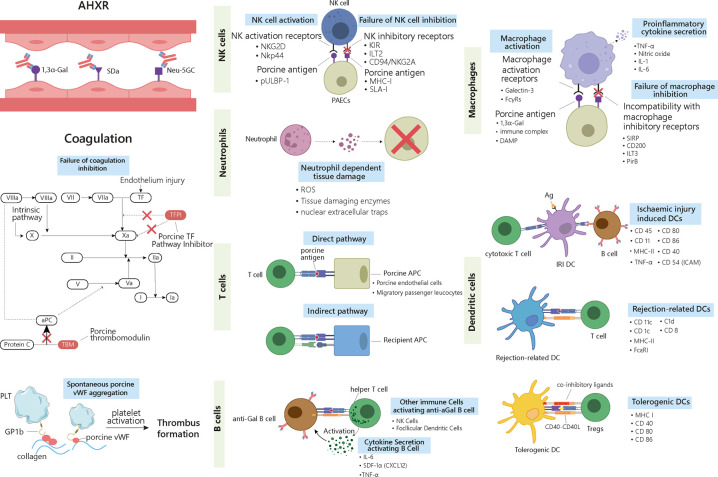
Transplantation is often the last resort for end-stage organ failures, e.g., kidney, liver, heart, lung, and pancreas. The shortage of donor organs is the main limiting factor for successful transplantation in humans. Except living donations, other alternatives are needed, e.g., xenotransplantation of pig organs. However, immune rejection remains the major challenge to overcome in xenotransplantation. There are three different xenogeneic types of rejections, based on the responses and mechanisms involved. It includes hyperacute rejection (HAR), delayed xenograft rejection (DXR) and chronic rejection. DXR, sometimes involves acute humoral xenograft rejection (AHR) and cellular xenograft rejection (CXR), which cannot be strictly distinguished from each other in pathological process. In this review, we comprehensively discussed the mechanism of these immunological rejections and summarized the strategies for preventing them, such as generation of gene knock out donors by different genome editing tools and the use of immunosuppressive regimens. We also addressed organ-specific barriers and challenges needed to pave the way for clinical xenotransplantation. Taken together, this information will benefit the current immunological research in the field of xenotransplantation.
Keywords: Xenotransplantation; chronic rejection; delayed xenograft rejection; glucocorticoids; hyperacute rejection; immunosuppressants.
Copyright © 2022 Zhou, Li, Wang, Zhang, Geng, Deng, Cheng and Wang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- D. Working Group on Incentives for Living. Matas AJ, Satel S, Munn S, Richards JR, Tan-Alora A, et al. Danguilan: Incentives for organ donation: proposed standards for an internationally acceptable system. Am J Transplant (2012) 12(2):306–12. doi: 10.1111/j.1600-6143.2011.03881.x - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous