

Cardiac manifestations in a Chinese cohort of fetuses from mothers with anti-Ro and anti-La antibodies
- PMID: 35967560
- PMCID: PMC9371606
- DOI: 10.3389/fped.2022.904138
Cardiac manifestations in a Chinese cohort of fetuses from mothers with anti-Ro and anti-La antibodies
Abstract
Objectives: To analyze the clinical characteristics, echocardiographic features, and prognosis of fetuses based on three groups of cardiac manifestations associated with maternal anti-Ro and anti-La antibodies in China. This study included three groups: the isolated-arrhythmia, isolated-endocardial fibroelastosis (EFE), and mixed groups.
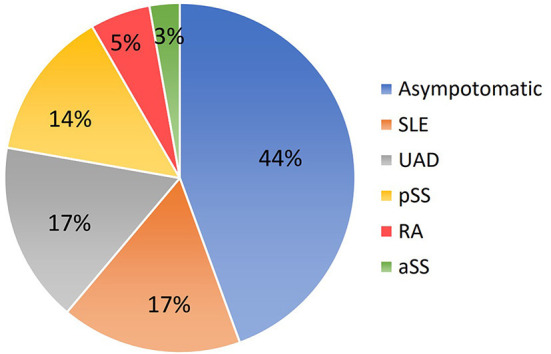
Methods: We prospectively evaluated 36 fetuses with cardiac manifestations due to maternal anti-Ro and anti-La antibodies from our center between 2016 and 2020 in China. Clinical and echocardiographic data were collected.
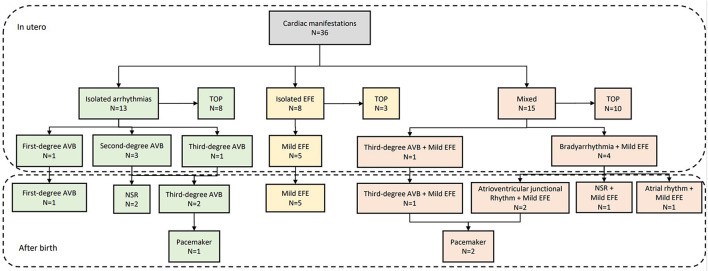
Results: There were 13 patients (36%) in the isolated-arrhythmia group, eight (22%) in the isolated-EFE group, and 15 (42%) in the mixed group. All patients in the isolated-EFE group presented with mild EFE. Severe EFE was identified in four patients (27%) in the mixed group. Atrioventricular block (AVB) was more common in the isolated-arrhythmia group (13, 100%) than in the mixed group (6, 40%; p = 0.001). Moderate-severe mitral regurgitation (p = 0.006), dilated cardiomyopathy (DCM, p = 0.017), and low cardiovascular profile scores (p = 0.013) were more common in the mixed group than in the other two groups. Twenty-one mothers decided to terminate the pregnancy and 15 fetuses were born with regular perinatal treatment. They all survived at 1 year of age. One patient in the isolated-arrhythmia group and two in the mixed group required a pacemaker due to third-degree AVB or atrioventricular junctional rhythm. Five patients in the isolated-EFE group and five in the mixed group had no DCM or heart failure and the location of mild EFE was significantly reduced.
Conclusion: Fetal cardiac manifestations due to maternal anti-Ro and anti-La antibodies can be divided into three groups, i.e., the isolated-arrhythmia, isolated-EFE, and mixed groups. AVB usually occurs in the isolated-arrhythmia group. Severe EFE, moderate-severe mitral regurgitation, and DCM mainly appear in the mixed group. Location of mild EFE significantly reduces after birth and the outcome of fetuses with mild EFE depends on the presence of arrhythmia and its subtypes.
Keywords: anti-Ro antibodies; atrioventricular block; echocardiography; endocardial fibroelastosis; prenatal diagnosis.
Copyright © 2022 Wang, Liu, Han, Li, Zhao, Sun, Han, Zeng, Tian, Zhao and He.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Patterns of endocardial fibroelastosis without atrioventricular block in fetuses exposed to anti-Ro/SSA antibodies.Ultrasound Obstet Gynecol. 2023 Jul;62(1):148-151. doi: 10.1002/uog.26181. Ultrasound Obstet Gynecol. 2023. PMID: 36806323
-
Maternal anti-Ro and anti-La antibody-associated endocardial fibroelastosis.Circulation. 2002 Feb 19;105(7):843-8. doi: 10.1161/hc0702.104182. Circulation. 2002. PMID: 11854125
-
Endocardial fibroelastosis associated with maternal anti-Ro and anti-La antibodies in the absence of atrioventricular block.J Am Coll Cardiol. 2002 Aug 21;40(4):796-802. doi: 10.1016/s0735-1097(02)02004-1. J Am Coll Cardiol. 2002. PMID: 12204513
-
Endocardial Fibroelastosis as an Independent Predictor of Atrioventricular Valve Rupture in Maternal Autoimmune Antibody Exposed Fetus: A Systematic Review with Clinicopathologic Analysis.Diagnostics (Basel). 2023 Apr 20;13(8):1481. doi: 10.3390/diagnostics13081481. Diagnostics (Basel). 2023. PMID: 37189582 Free PMC article. Review.
-
Prevention of complete heart block in children of mothers with anti-SSA/Ro and anti-SSB/La autoantibodies: detection and treatment of first-degree atrioventricular block.Curr Opin Rheumatol. 2009 Sep;21(5):478-82. doi: 10.1097/BOR.0b013e32832ed817. Curr Opin Rheumatol. 2009. PMID: 19584727 Review.
Cited by
-
Ultrasonographic characterization and prognostic follow-up of fetal cardiac involvement in maternal immune diseases.Front Med (Lausanne). 2025 Jun 16;12:1564873. doi: 10.3389/fmed.2025.1564873. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40589968 Free PMC article.
References
-
- Brucato A, Frassi M, Franceschini F, Cimaz R, Faden D, Pisoni MP, et al. . Risk of congenital complete heart block in newborns of mothers with anti-Ro/SSA antibodies detected by counterimmunoelectrophoresis: a prospective study of 100 women. Arthritis Rheum. (2001) 44:1832–5. 10.1002/1529-0131(200108)44:8<1832::AID-ART320>3.0.CO;2-C - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials