

Low-Cost "Telesimulation" Training Improves Real Patient Pediatric Shock Outcomes in India
- PMID: 35967566
- PMCID: PMC9364444
- DOI: 10.3389/fped.2022.904846
Low-Cost "Telesimulation" Training Improves Real Patient Pediatric Shock Outcomes in India
Abstract
Introduction: Pediatric shock, especially septic shock, is a significant healthcare burden in low-income countries. Early recognition and management of shock in children improves patient outcome. Simulation-based education (SBE) for shock recognition and prompt management prepares interdisciplinary pediatric emergency teams in crisis management. COVID-19 pandemic restrictions on in-person simulation led us to the development of telesimulation for shock. We hypothesized that telesimulation training would improve pediatric shock recognition, process of care, and patient outcomes in both simulated and real patient settings.
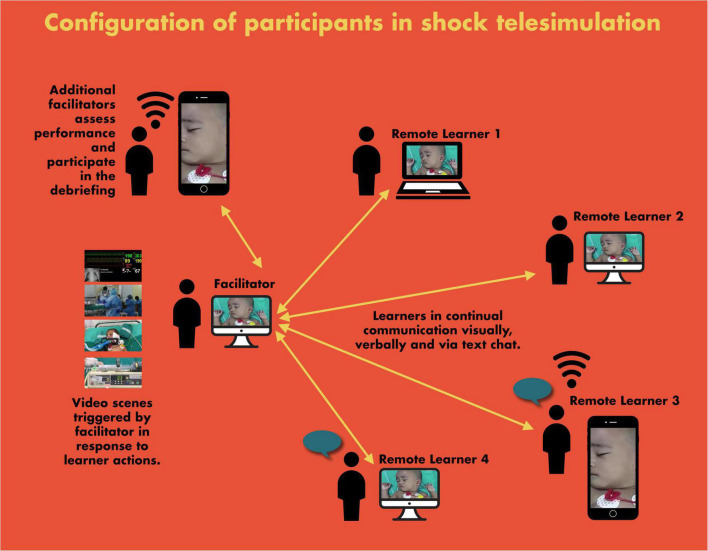
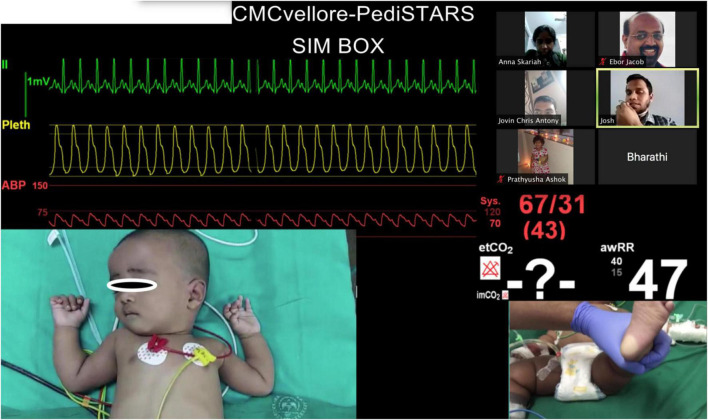
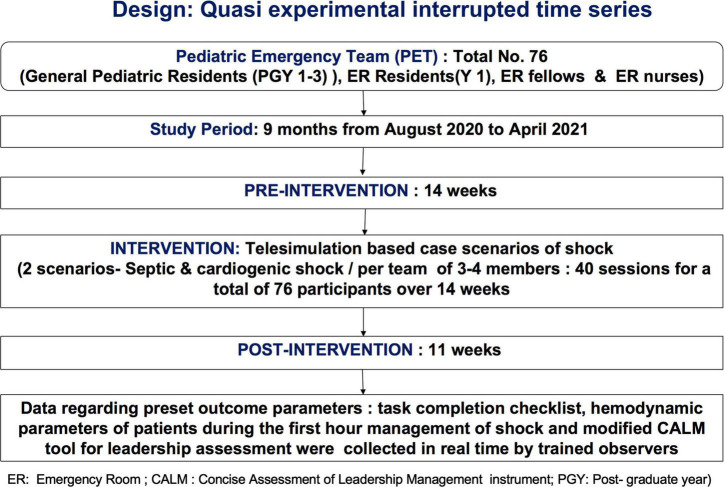
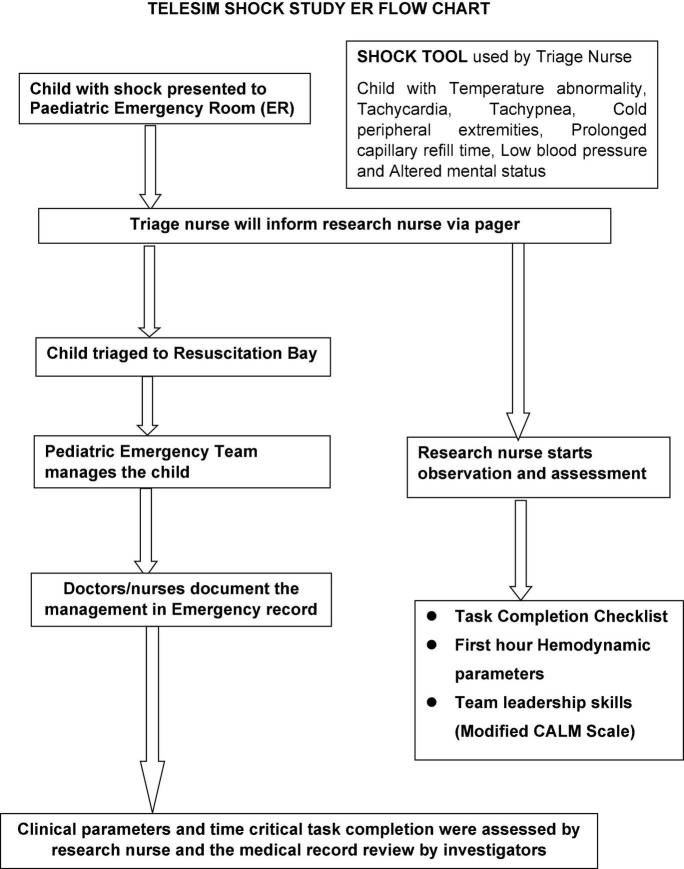
Materials and methods: We conducted a prospective quasi-experimental interrupted time series cohort study over 9 months. We conducted 40 telesimulation sessions for 76 participants in teams of 3 or 4, utilizing the video telecommunication platform (Zoom©). Trained observers recorded time-critical interventions on real patients for the pediatric emergency teams composed of residents, fellows, and nurses. Data were collected on 332 pediatric patients in shock (72% of whom were in septic shock) before, during, and after the intervention. The data included the first hour time-critical intervention checklist, patient hemodynamic status at the end of the first hour, time for the resolution of shock, and team leadership skills in the emergency room.
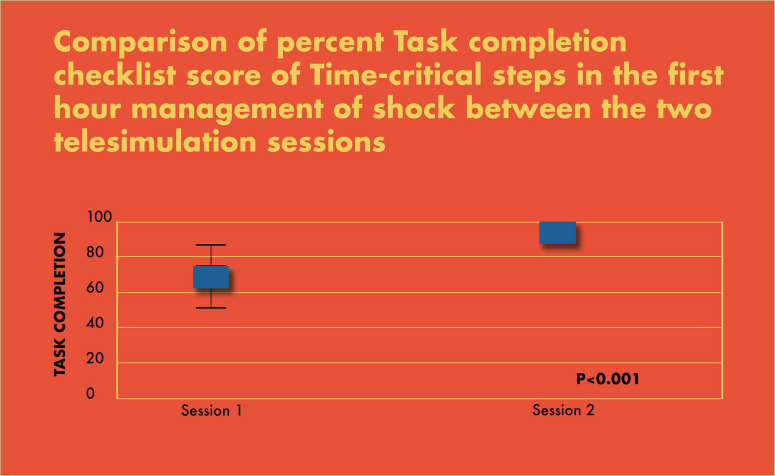
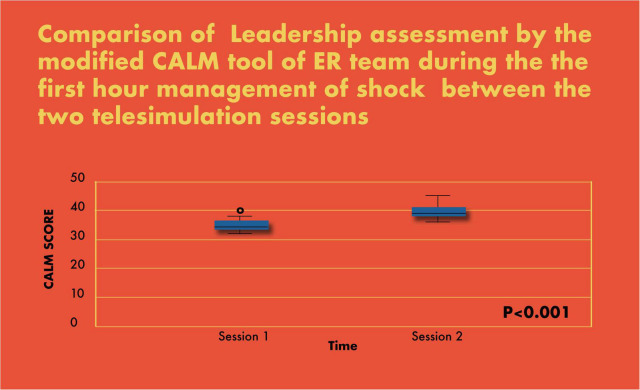
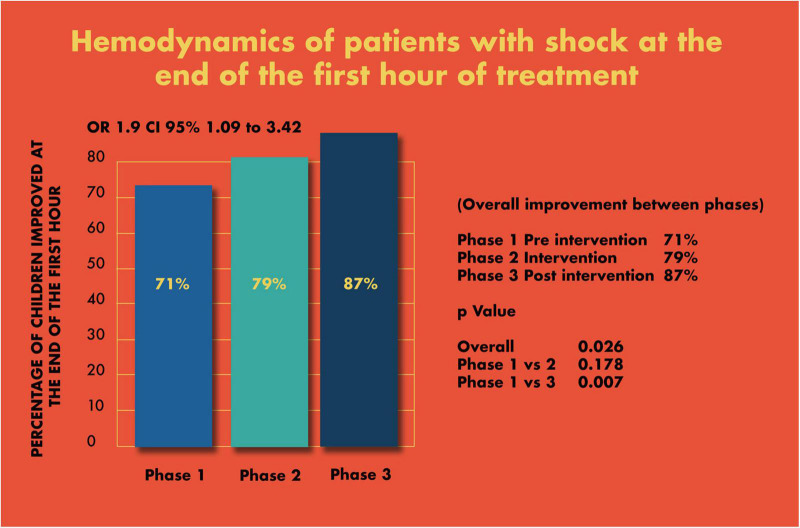
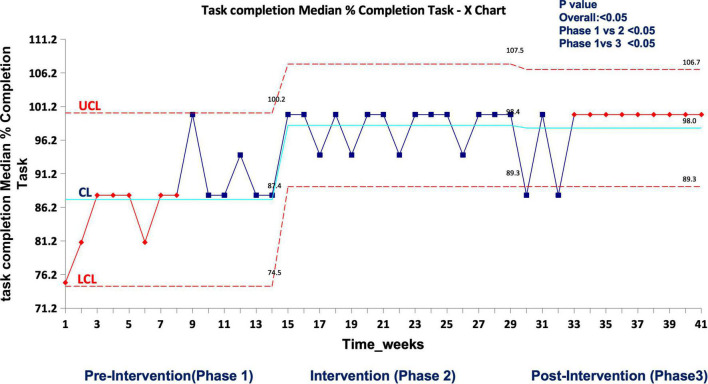
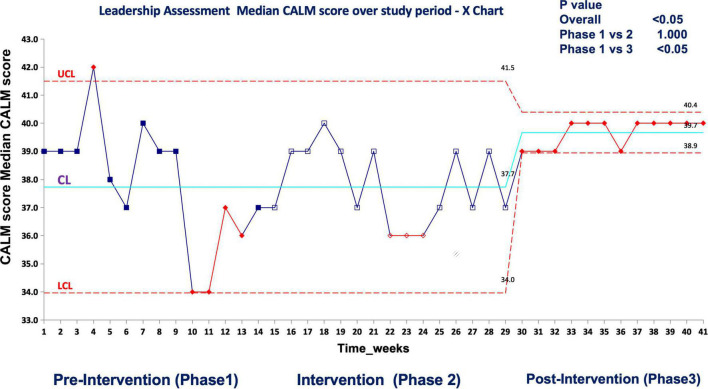
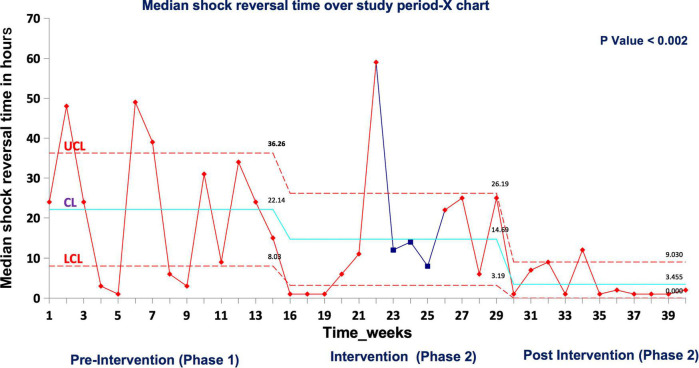
Results: There was a significant improvement in the percent completion of tasks by the pediatric emergency team in simulated scenarios (69% in scenario 1 vs. 93% in scenario 2; p < 0.001). In real patients, completion of tasks as per time-critical steps reached 100% during and after intervention compared to the pre-intervention phase (87.5%), p < 0.05. There was a significant improvement in the first hour hemodynamic parameters of shock patients: pre (71%), during (79%), and post (87%) intervention (p < 0.007 pre vs. post). Shock reversal time reduced from 24 h pre-intervention to 6 h intervention and to 4.5 h post intervention (p < 0.002). There was also a significant improvement in leadership performance assessed by modified Concise Assessment of Leader Management (CALM) instrument during the simulated (p < 0.001) and real patient care in post intervention (p < 0.05).
Conclusion: Telesimulation training is feasible and improved the process of care, time-critical interventions, leadership in both simulated and real patients and resolution of shock in real patients. To the best of our knowledge, this is one of the first studies where telesimulation has shown improvement in real patient outcomes.
Keywords: COVID-19 educational innovations; hotkeys; septic shock; simulation-based education; telesimulation.
Copyright © 2022 James, Vyasam, Venkatachalam, Sanseau, Cassidy, Ramachandra, Rebekah, Adhikari, Deutsch, Nishisaki and Nadkarni.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
Evaluating Emotional Outcomes of Medical Students in Pediatric Emergency Medicine Telesimulation.Children (Basel). 2023 Jan 15;10(1):169. doi: 10.3390/children10010169. Children (Basel). 2023. PMID: 36670719 Free PMC article.
-
Development of a simulation curriculum to teach and assess advanced laparoscopic suturing skills using telesimulation: a feasibility study.Surg Endosc. 2022 Jul;36(7):5483-5490. doi: 10.1007/s00464-021-08880-6. Epub 2022 Jan 8. Surg Endosc. 2022. PMID: 34997338 Free PMC article.
-
The sim must go on: adapting resident education to the COVID-19 pandemic using telesimulation.Adv Simul (Lond). 2020 Sep 29;5:26. doi: 10.1186/s41077-020-00146-w. eCollection 2020. Adv Simul (Lond). 2020. PMID: 32999738 Free PMC article.
-
Telesimulation in healthcare education: A scoping review.Nurse Educ Today. 2023 Jul;126:105805. doi: 10.1016/j.nedt.2023.105805. Epub 2023 Mar 31. Nurse Educ Today. 2023. PMID: 37062239
-
Mannequin-based Telesimulation: Increasing Access to Simulation-based Education.Acad Emerg Med. 2018 Feb;25(2):144-147. doi: 10.1111/acem.13299. Epub 2017 Oct 4. Acad Emerg Med. 2018. PMID: 28846175
Cited by
-
Breaking barriers in establishing simulation in India-A collaborative approach by pediatric simulation training and research society (PediSTARS).Front Pediatr. 2022 Sep 21;10:927711. doi: 10.3389/fped.2022.927711. eCollection 2022. Front Pediatr. 2022. PMID: 36210949 Free PMC article.
-
Exploring the use of low-cost simulation in nursing education: a scoping review.BMJ Open. 2025 Jul 17;15(7):e099968. doi: 10.1136/bmjopen-2025-099968. BMJ Open. 2025. PMID: 40675641 Free PMC article.
-
Barriers and facilitators when seeking healthcare for septic children in Ghana: a single-centre qualitative study of patient caregivers and emergency department clinicians.BMJ Paediatr Open. 2024 Aug 21;8(1):e002814. doi: 10.1136/bmjpo-2024-002814. BMJ Paediatr Open. 2024. PMID: 39174034 Free PMC article.
-
Annenberg Hotkeys: A Free, Simple, Interactive Learning Platform.Cureus. 2025 Mar 29;17(3):e81412. doi: 10.7759/cureus.81412. eCollection 2025 Mar. Cureus. 2025. PMID: 40296927 Free PMC article.
References
-
- Institute of Medicine. Emergency Care for Children: Growing Pains. Washington, DC: The National Academies Press; (2007).
-
- Remick K, Gausche-Hill M, Joseph MM, Brown K, Snow SK, Wright JL, et al. Pediatric readiness in the emergency department. Pediatrics. (2018) 142:e20182459. - PubMed
-
- Viana ME, Valete CO, Sgorlon G, Vieira JA, Currais JC, Martins MP, et al. An international perspective on the treatment of pediatric shock: the Brazilian experience. New Horiz. (1998) 6:226–34. - PubMed
LinkOut - more resources
Full Text Sources