

The Role of Targeted Osmotic Lysis in the Treatment of Advanced Carcinoma in Companion Animals: A Case Series
- PMID: 35967596
- PMCID: PMC9363929
- DOI: 10.1155/2022/2747108
The Role of Targeted Osmotic Lysis in the Treatment of Advanced Carcinoma in Companion Animals: A Case Series
Abstract
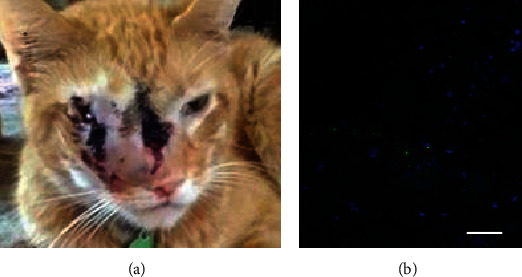
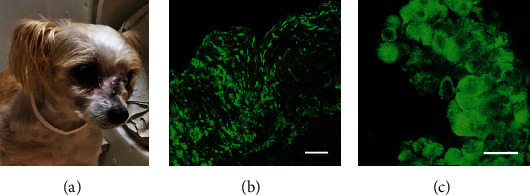
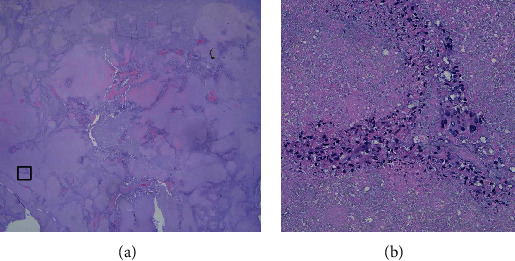
Background: Targeted osmotic lysis (TOL) is a novel technology that involves concomitant stimulation of voltage-gated sodium channels (VGSCs) and the pharmacological blockade of Na+, K+-ATPase causing lysis of highly malignant cancer cells. Hypothesis/Objectives. TOL offers an option for treating advanced carcinomas in companion animals. Animals. Two cats and 2 dogs that presented to veterinary hospitals for evaluation and treatment of one of several forms of carcinoma.
Methods: Digoxin was administered to achieve steady-state, therapeutic concentrations. The animals were then exposed to pulsed electric field stimulation. Pre- and posttreatment assessments of tumor size and quality of life were compared. The treatment frequency and survivability varied, based on the patient's premorbid functioning and response to treatment.
Results: Regardless of cancer type, TOL consistently increased survival beyond expected, often improving, but without compromising of quality of life. Conclusions and Clinical Importance. TOL warrants consideration as an option for managing advanced carcinomas.
Copyright © 2022 Harry J. Gould III et al.
Conflict of interest statement
H.J.G., P.R.M, and D.P. are cofounders and managing members of Oleander Medical Technologies, L.LC.
Figures










Similar articles
-
Targeted Osmotic Lysis of Highly Invasive Breast Carcinomas Using Pulsed Magnetic Field Stimulation of Voltage-Gated Sodium Channels and Pharmacological Blockade of Sodium Pumps.Cancers (Basel). 2020 May 31;12(6):1420. doi: 10.3390/cancers12061420. Cancers (Basel). 2020. PMID: 32486340 Free PMC article.
-
Emergency Use of Targeted Osmotic Lysis for the Treatment of a Patient with Aggressive Late-Stage Squamous Cell Carcinoma of the Cervix.Curr Oncol. 2021 Jun 8;28(3):2115-2122. doi: 10.3390/curroncol28030196. Curr Oncol. 2021. PMID: 34201380 Free PMC article.
-
Safety evaluation of targeted osmotic lysis therapy in Beagles.Am J Vet Res. 2024 Dec 16;86(2):ajvr.24.09.0284. doi: 10.2460/ajvr.24.09.0284. Print 2025 Feb 1. Am J Vet Res. 2024. PMID: 39681070
-
Targeted Osmotic Lysis: A Novel Approach to Targeted Cancer Therapies.Biomedicines. 2022 Apr 2;10(4):838. doi: 10.3390/biomedicines10040838. Biomedicines. 2022. PMID: 35453588 Free PMC article. Review.
-
Disease Risk Assessments Involving Companion Animals: an Overview for 15 Selected Pathogens Taking a European Perspective.J Comp Pathol. 2016 Jul;155(1 Suppl 1):S75-97. doi: 10.1016/j.jcpa.2015.08.003. Epub 2015 Sep 28. J Comp Pathol. 2016. PMID: 26422413 Review.
Cited by
-
Cancer as a Channelopathy-Appreciation of Complimentary Pathways Provides a Different Perspective for Developing Treatments.Cancers (Basel). 2022 Sep 23;14(19):4627. doi: 10.3390/cancers14194627. Cancers (Basel). 2022. PMID: 36230549 Free PMC article. Review.
-
Systemic Mechanisms of Ionic Regulation in Carcinogenesis.Cancers (Basel). 2025 Jan 17;17(2):286. doi: 10.3390/cancers17020286. Cancers (Basel). 2025. PMID: 39858068 Free PMC article. Review.
References
-
- Fetch a Cure. Facts. 2021, https://fetchacure.org/resource-library/facts/
-
- Paul D., Maggi P., Piero F. D., et al. Targeted osmotic lysis of highly invasive breast carcinomas using pulsed magnetic field stimulation of voltage-gated sodium channels and pharmacological blockade of sodium pumps. Cancers . 2020;12(6):1420–1433. doi: 10.3390/cancers12061420. - DOI - PMC - PubMed
-
- Djamgoz M. B., Onkal R. Persistent current blockers of voltage-gated sodium channels: a clinical opportunity for controlling metastatic disease. Recent Patents on Anti-Cancer Drug Discovery . 2013;8(1):66–84. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous