

A Novel Osteoporosis Screening Protocol to Identify Orthopedic Surgery Patients for Preoperative Bone Health Optimization
- PMID: 35967749
- PMCID: PMC9364193
- DOI: 10.1177/21514593221116413
A Novel Osteoporosis Screening Protocol to Identify Orthopedic Surgery Patients for Preoperative Bone Health Optimization
Abstract
Introduction: Osteoporosis is highly prevalent in elective orthopedic surgery. While preoperative bone health optimization decreases osteoporosis-related complications, there is an unmet need to establish who may benefit from preoperative dual-energy x-ray absorptiometry (DXA). This study assesses a novel, simple screening protocol to identify orthopedic surgical patients for preoperative DXA.
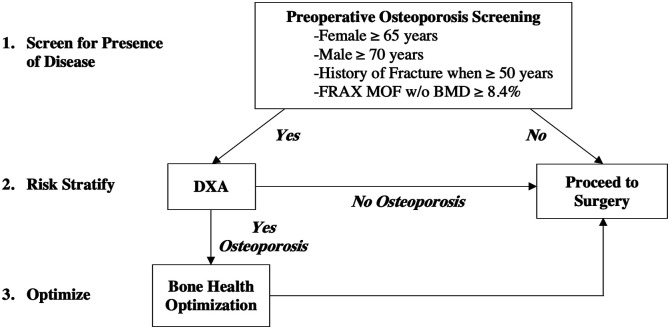
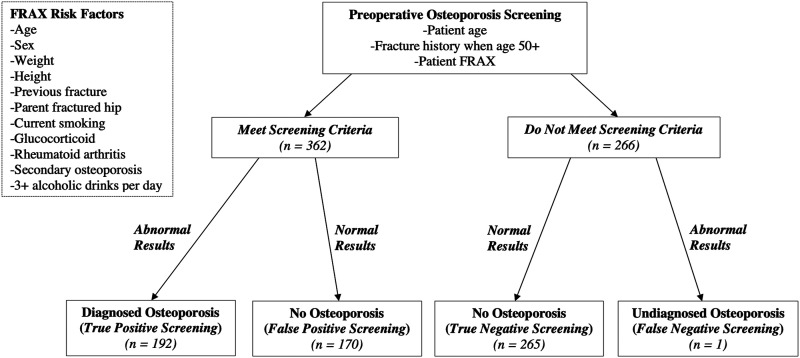
Materials/methods: This retrospective cohort study included 628 patients undergoing total knee, hip, or shoulder arthroplasty or thoracolumbar spine fusion. Inclusion criteria were ≥40 years undergoing primary elective surgery. Screening criteria defining who should obtain DXA due to high osteoporosis risk included: female ≥65, male ≥70, fracture history when ≥50 years, or FRAX major osteoporotic fracture risk (without bone mineral density [BMD]-adjustments) ≥8.4%. Osteoporosis was defined by World Health Organization criteria [T-score ≤ -2.5], clinical National Osteoporosis Foundation (NOF) criteria [T-score ≤ -2.5, elevated BMD-adjusted FRAX risk, or prior hip/spine fracture], and modified clinical criteria [NOF criteria simplified to include any non-traumatic prior fracture and FRAX without BMD].
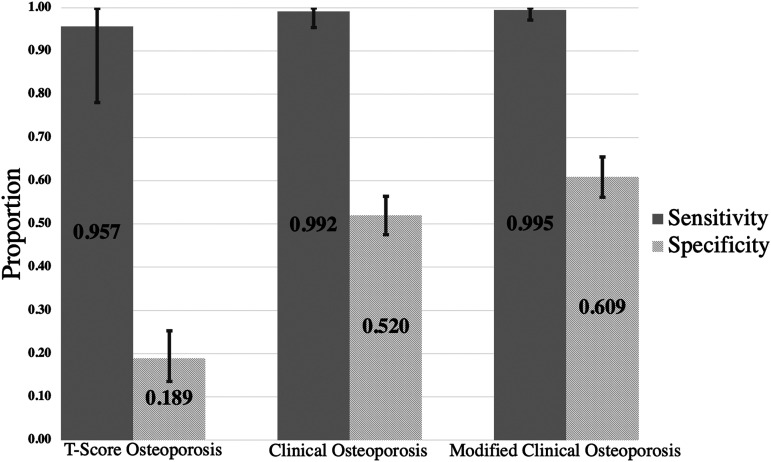
Results: The study included 100 TKAs, 100 THAs, 251 TSAs, and 177 spine fusions, average age 65.6 ± 9.8. DXA was available for 209 patients. Screening criteria recommending DXA was met by 362 patients. For those with DXA, screening sensitivity was .96 (CI: .78 to .99) and specificity was .19 (CI: .14 to .25) for identifying T-score osteoporosis. Similar sensitivity of .99 (CI: .91 to .99) and specificity of .61 (CI: .56 to .66) were found for modified clinical osteoporosis. For modified clinical osteoporosis, 192 patients with osteoporosis met criteria (true pos.), 1 patient with osteoporosis did not meet criteria (false neg.), 170 patients without osteoporosis met criteria (false pos.), and 265 patients without osteoporosis did not meet criteria (true neg.).
Discussion/conclusion: A simple screening protocol identifies orthopedic surgical candidates at risk of T-score or clinical osteoporosis for preoperative DXA with high sensitivity.
Keywords: adult reconstructive surgery; bone health optimization; bone health screening; bone mineral density; fragility fractures; metabolic bone disorders; osteoporosis; spine surgery.
© The Author(s) 2022.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
Proposed bone health screening protocol to identify total knee arthroplasty patients for preoperative DXA.Osteoporos Int. 2023 Jan;34(1):171-177. doi: 10.1007/s00198-022-06585-7. Epub 2022 Nov 3. Osteoporos Int. 2023. PMID: 36326846
-
Preoperative bone health assessment and optimization in spine surgery.Neurosurg Focus. 2020 Aug;49(2):E2. doi: 10.3171/2020.5.FOCUS20255. Neurosurg Focus. 2020. PMID: 32738805
-
Utilization of DXA Bone Mineral Densitometry in Ontario: An Evidence-Based Analysis.Ont Health Technol Assess Ser. 2006;6(20):1-180. Epub 2006 Nov 1. Ont Health Technol Assess Ser. 2006. PMID: 23074491 Free PMC article.
-
Use of Bone Health Evaluation in Orthopedic Surgery: 2019 ISCD Official Position.J Clin Densitom. 2019 Oct-Dec;22(4):517-543. doi: 10.1016/j.jocd.2019.07.013. Epub 2019 Aug 16. J Clin Densitom. 2019. PMID: 31519473 Review.
-
Bone health in childhood and adolescence: an overview on dual-energy X-ray absorptiometry scanning, fracture surveillance and bisphosphonate therapy for low-middle-income countries.Front Endocrinol (Lausanne). 2023 Apr 17;14:1082413. doi: 10.3389/fendo.2023.1082413. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 37139332 Free PMC article. Review.
Cited by
-
Utility of osteoporosis screening based on estimation of bone mineral density using bidirectional chest radiographs with deep learning models.Front Med (Lausanne). 2025 Mar 26;12:1499670. doi: 10.3389/fmed.2025.1499670. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40206487 Free PMC article.
-
The Role of Osteoporosis in Total Hip Arthroplasty Periprosthetic Fractures and Current Management Strategies: a Review.Curr Osteoporos Rep. 2025 Jun 23;23(1):29. doi: 10.1007/s11914-025-00922-5. Curr Osteoporos Rep. 2025. PMID: 40551042 Review.
-
Vertebral bone quality score as a new tool for osteoporosis diagnosis in patients undergoing lumbosacral fusion surgery: a single center cohort study.Eur J Transl Myol. 2024 Sep 16;34(4):12311. doi: 10.4081/ejtm.2024.12311. Eur J Transl Myol. 2024. PMID: 39283159 Free PMC article.
-
Osteoporosis in the setting of knee arthroplasty: a narrative review.Arthroplasty. 2024 Oct 2;6(1):50. doi: 10.1186/s42836-024-00273-z. Arthroplasty. 2024. PMID: 39354637 Free PMC article. Review.
-
The role of humerus cortical thickness in predicting osteoporosis in MR imaging.Shoulder Elbow. 2024 Sep 11:17585732241279090. doi: 10.1177/17585732241279090. Online ahead of print. Shoulder Elbow. 2024. PMID: 39545007 Free PMC article.
References
-
- Maier GS, Kolbow K, Lazovic D, Maus U. The importance of bone mineral density in hip arthroplasty: Results of a survey asking orthopaedic surgeons about their opinions and attitudes concerning osteoporosis and hip arthroplasty. Advances in Orthopedics. 2016;2016:1-5. doi:10.1155/2016/8079354 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
