

Successful Treatment of Non-Langerhans Cell Histiocytosis With Topical Rapamycin in Two Pediatric Cases
- PMID: 35967913
- PMCID: PMC9365013
- DOI: 10.2147/CCID.S375995
Successful Treatment of Non-Langerhans Cell Histiocytosis With Topical Rapamycin in Two Pediatric Cases
Abstract
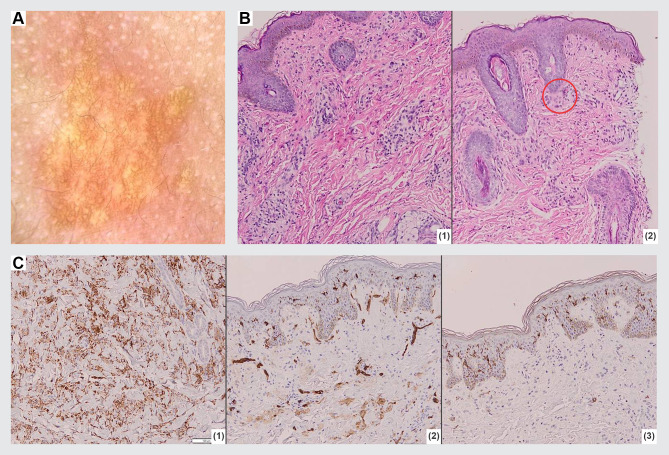
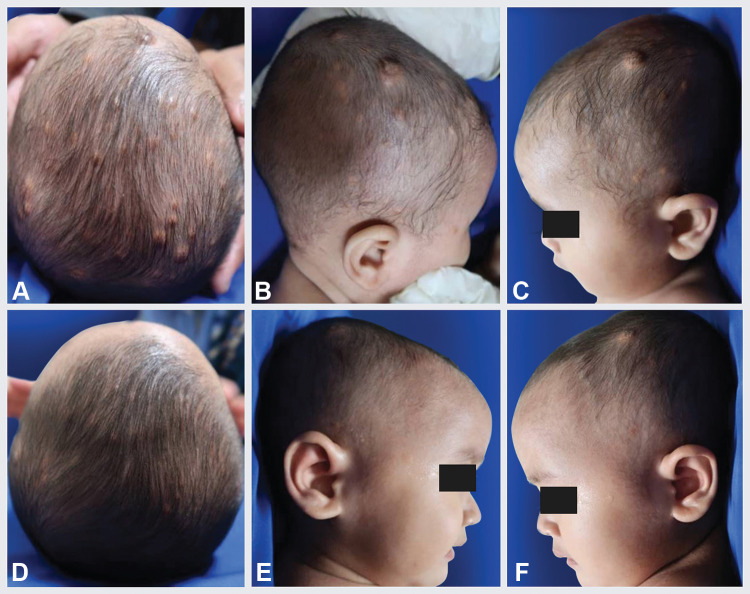
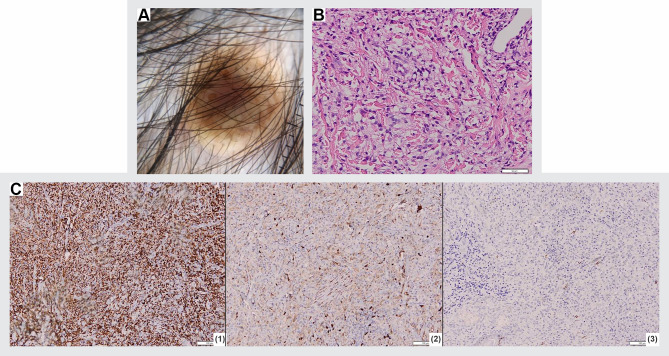
Non-Langerhans cell histiocytosis (non-LCH) is a group of diseases characterized by the proliferation of histiocytes in tissues that is excluded from the diagnostic criteria for LCH. Juvenile xanthogranuloma (JXG) and benign cephalic histiocytosis (BCH) are the most common types of cutaneous non-LCH. These two diseases share similarities in both clinical and histological features, therefore, they can be difficult to differentiate. Thorough physical, dermoscopic, and histopathological examinations are required to distinguish between JXG and BCH. We hereby present two rare cases of non-LCH in pediatric patients, presented with JXG and BCH. The dermoscopic examination of both cases showed a setting-sun appearance, while the histopathological examination revealed Touton giant cells in the JXG case, and massive lymphocyte infiltration in the BCH case. Both patients were treated with 1% topical rapamycin in a split-side comparison for the first 12 weeks, followed by applications on both sides for a total duration of 24 weeks. As a result, there was a significant reduction in the size of the lesion, leading to patient's satisfaction. Rapamycin is an immunosuppressive agent with antineoplastic activity. Rapamycin can be used as an alternative non-invasive topical treatment option for JXG and BCH. However, long-term observations are required to assess its effectiveness and side effects.
Keywords: benign cephalic histiocytosis; dermoscopy examination; histopathological examination; juvenile xanthogranuloma; non-Langerhans cell histiocytosis.
© 2022 Effendi et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures

Similar articles
-
Generalized Eruptive Histiocytosis or Juvenile Xanthogranuloma: A Clinicopathological Conundrum of Coexistence or Xanthomatization.Indian Dermatol Online J. 2024 Jul 5;15(5):828-833. doi: 10.4103/idoj.idoj_540_23. eCollection 2024 Sep-Oct. Indian Dermatol Online J. 2024. PMID: 39359292 Free PMC article.
-
Juvenile xanthogranuloma as a sequel to Langerhans cell histiocytosis: a report of three cases.Clin Exp Dermatol. 2001 Jul;26(5):391-4. doi: 10.1046/j.1365-2230.2001.00842.x. Clin Exp Dermatol. 2001. PMID: 11488823
-
Benign cephalic histiocytosis progressing into juvenile xanthogranuloma: a non-Langerhans cell histiocytosis transforming under the influence of a virus?Am J Dermatopathol. 2000 Feb;22(1):70-4. doi: 10.1097/00000372-200002000-00014. Am J Dermatopathol. 2000. PMID: 10698221
-
Structural correlations between dermoscopic and histopathological features of juvenile xanthogranuloma.J Eur Acad Dermatol Venereol. 2011 Mar;25(3):259-63. doi: 10.1111/j.1468-3083.2010.03819.x. J Eur Acad Dermatol Venereol. 2011. PMID: 20698915 Review.
-
Oral juvenile xanthogranuloma in a child: Clinical, histological and immunohistochemical profile of a rare entity.J Cutan Pathol. 2018 Jul;45(7):515-521. doi: 10.1111/cup.13152. Epub 2018 May 9. J Cutan Pathol. 2018. PMID: 29624716 Review.
Cited by
-
A late presentation of benign cephalic histiocytosis.JAAD Case Rep. 2024 Nov 23;61:159-160. doi: 10.1016/j.jdcr.2024.10.030. eCollection 2025 Jul. JAAD Case Rep. 2024. PMID: 40678378 Free PMC article. No abstract available.
-
mTORC1 activity negatively regulates human hair follicle growth and pigmentation.EMBO Rep. 2023 Jul 5;24(7):e56574. doi: 10.15252/embr.202256574. Epub 2023 May 22. EMBO Rep. 2023. PMID: 37212043 Free PMC article.
-
Frequent detection of genetic aberrations reveals novel pathogenesis and treatment modalities in systemic juvenile xanthogranuloma.Pediatr Investig. 2023 Aug 28;7(3):212-215. doi: 10.1002/ped4.12398. eCollection 2023 Sep. Pediatr Investig. 2023. PMID: 37736360 Free PMC article. No abstract available.
References
-
- Schmieder A, Goerdt S, Utikal J, et al. Histiocytosis. In: Kang S, Amagai M, Bruckner AL, Enk AH, Margolis DJ, McMichael AJ, editors. Fitzpatrick’s Dermatology. 1, 9th. New York: Mc Graw Hill; 2019:2018–2041.
-
- Ratzinger G, Zelger BWH. Juvenile Xanthogranuloma and Other Non-Langerhans Cell Histiocytoses. In: Hoeger P, Kinsler V, Yan A, editors. Harper’s Textbook of Pediatric Dermatology. Juvenile Xanthogranuloma and Other Non-Langerhans Cell Histiocytoses. Pondicherry: Wiley-Blackwell; 2020:1078–1096.
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
