

Clinico-bacterial and prognostic factors in patients with suspected blood stream infection and elevated serum procalcitonin levels
- PMID: 35967939
- PMCID: PMC9350570
- DOI: 10.18999/nagjms.84.2.230
Clinico-bacterial and prognostic factors in patients with suspected blood stream infection and elevated serum procalcitonin levels
Abstract
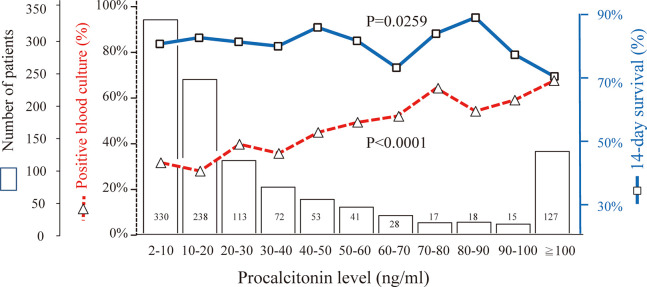
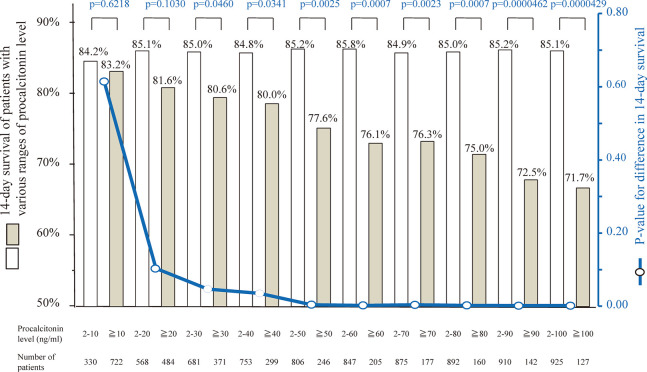
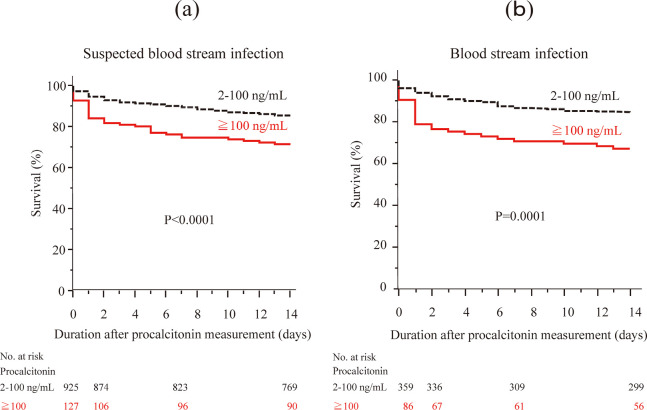
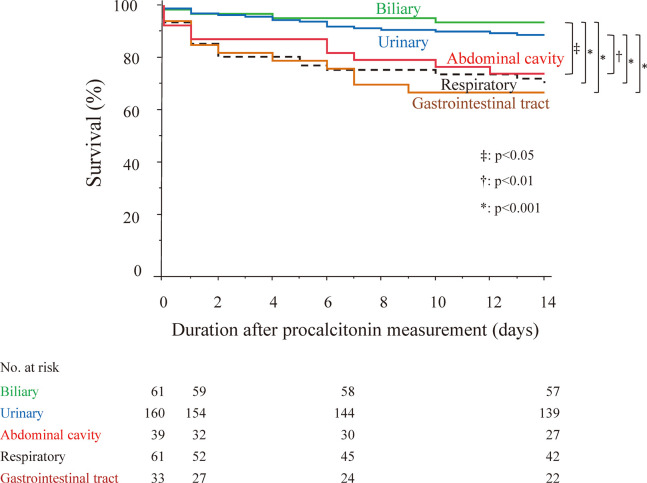
This study determined prognostic factors by comparing clinico-bacterial factors based on significant elevated serum procalcitonin levels in patients with suspected bloodstream infection (BSI). We retrospectively analyzed the medical records of 1,052 patients (age ≥16 years) with fever (temperature ≥38°C) and serum procalcitonin levels of ≥2.0 ng/mL, and blood culture results. The optimal cutoff value of the significant elevation of procalcitonin was determined using the minimum P-value approach. Clinico-bacterial factors were analyzed per the procalcitonin levels, and significant independent factors for short-term survival were investigated in 445 patients with BSI. Patients with suspected BSI were aged, on average, 72.3 ± 15.1 years, and the incidence of positive blood culture was 42.3%; and the 14-day survival was 83.4%. Procalcitonin ≥100 ng/mL was the most significant predictor for survival. Multivariate analysis in patients with suspected BSI showed that estimated glomerular filtration rate (eGFR) <30 mL/min/1.73 m2 and procalcitonin ≥100 ng/mL were significant independent unfavorable prognostic factors. Microorganisms were similar between patients with procalcitonin level 2-99 ng/mL (n=359) and those with ≥100 ng/mL (n=86). Multivariate analysis in patients with BSI showed that eGFR <30 mL/min/1.73 m2, procalcitonin ≥100 ng/mL, and primary infectious foci were significant independent prognostic factors. Patients with foci in the gastrointestinal tract and respiratory system had unfavorable 14-day survival. In conclusions, eGFR <30 mL/min/1.73 m2 and procalcitonin ≥100 ng/mL were significant independent unfavorable prognostic factors for suspected BSI. Primary infectious foci (gastrointestinal tract and respiratory system) were associated with unfavorable short-term survival in patients with positive blood culture.
Keywords: blood culture; bloodstream infection; procalcitonin; renal function; survival.
Conflict of interest statement
There are no potential conflicts of interest to declare, with regard to the research, authorship, and publication of this article.
Figures
Similar articles
-
Procalcitonin as a marker for the detection of bacteremia and sepsis in the emergency department.Am J Clin Pathol. 2011 Feb;135(2):182-9. doi: 10.1309/AJCP1MFYINQLECV2. Am J Clin Pathol. 2011. PMID: 21228358
-
Clinical value of procalcitonin for suspected nosocomial bloodstream infection.Korean J Intern Med. 2018 Jan;33(1):176-184. doi: 10.3904/kjim.2016.119. Epub 2017 Nov 8. Korean J Intern Med. 2018. PMID: 29108401 Free PMC article.
-
The ability of Procalcitonin, lactate, white blood cell count and neutrophil-lymphocyte count ratio to predict blood stream infection. Analysis of a large database.J Crit Care. 2020 Dec;60:135-139. doi: 10.1016/j.jcrc.2020.07.026. Epub 2020 Aug 8. J Crit Care. 2020. PMID: 32799183
-
Clinical value of procalcitonin for patients with suspected bloodstream infection.Am J Clin Pathol. 2014 Jan;141(1):43-51. doi: 10.1309/AJCP4GV7ZFDTANGC. Am J Clin Pathol. 2014. PMID: 24343736
-
Procalcitonin as an early marker of infection in neonates and children.Lancet Infect Dis. 2004 Oct;4(10):620-30. doi: 10.1016/S1473-3099(04)01146-6. Lancet Infect Dis. 2004. PMID: 15451490 Review.
Cited by
-
Development and Validation of a Prognostic Model for Multi-Drug-Resistant Non-Hospital-Acquired Bloodstream Infection.Antibiotics (Basel). 2023 May 24;12(6):955. doi: 10.3390/antibiotics12060955. Antibiotics (Basel). 2023. PMID: 37370274 Free PMC article.
-
Clinical features, procalcitonin concentration, and bacterial infection in febrile hospitalized cancer patients: a descriptive study and association analysis.Support Care Cancer. 2025 Feb 4;33(2):148. doi: 10.1007/s00520-025-09216-z. Support Care Cancer. 2025. PMID: 39904763
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous