

Single-Port Cholecystectomy for Cholecystitis Versus Non-Cholecystitis
- PMID: 35967963
- PMCID: PMC9355797
- DOI: 10.4293/JSLS.2022.00020
Single-Port Cholecystectomy for Cholecystitis Versus Non-Cholecystitis
Abstract
Background and objectives: To assess the safety and efficacy of single-port laparoscopic cholecystectomy (SPLC) for the treatment of symptomatic cholelithiasis in different gallbladder pathologic conditions.
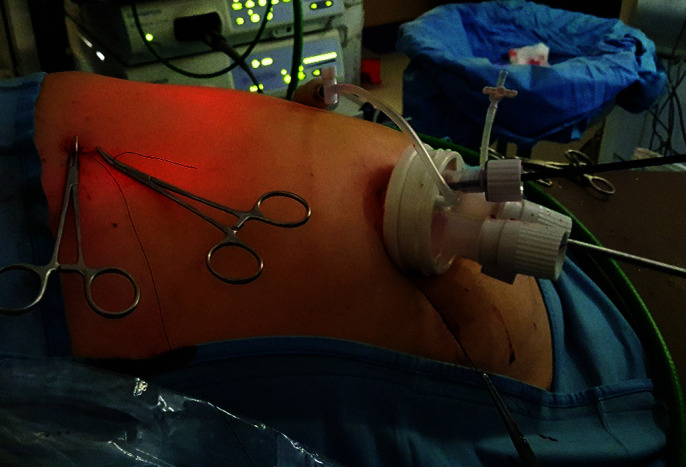
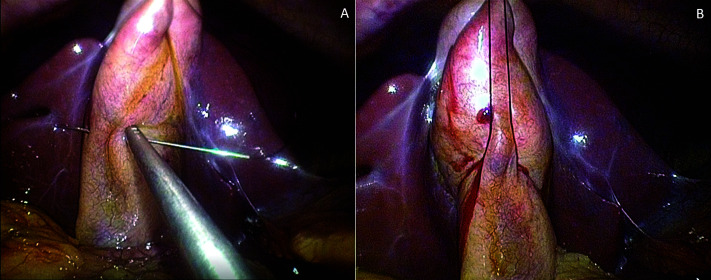
Methods: All patients who underwent SPLC in our department between October 1, 2017 and March 31, 2020 were registered consecutively in a prospective database. Patients' charts were retrospectively divided according to histological diagnosis: normal gallbladder (NG) (n = 13), chronic cholecystitis (CC) (n =47), and acute cholecystitis (AC) (n = 10). The parameters for assessing the procedure outcome included operative time, blood loss, use of additional trocars, conversion to laparotomy, intraoperative and postoperative complications, and length of hospital stay. Patient groups were statistically compared.
Results: Seventy patients underwent SPLC. Duration of surgery increased from NG (55 ± 22.7 min) to CC (70 ± 33.5 min), and to AC patients (110.5 ± 50.5 min), which is statistically significant (P = .001). Postoperative complication rates were 7.6% in NG patients, 17% in CC, and 30% in AC (P = .442). Length of hospitalization was shorter for NG patients (1.0 ± 0.6 days) versus CC (2.0 ± 1.1 days) and AC patients (2.0 ± 4.7 days), with statistical significance (P = .020). Multivariate analysis found that pathology type and the occurrence of postoperative complications were independent predictors for prolonged operative times and prolonged hospital stay, respectively.
Conclusion: SPLC is feasible for acute and chronic cholecystitis with good procedural outcomes. Since SPLC technique itself can be sometimes challenging with the existing technology, its application, especially in cases of acute cholecystitis, should be done with caution. Only prospective randomized studies on this approach for acute and chronic gallbladder diseases will assess the complete reliability of this technique.
Keywords: Acute cholecystitis; Chronic cholecystitis; Laparo-endoscopic single-site surgery; Single incision laparoscopic cholecystectomy; Single incision laparoscopic surgery; Single-port access surgery.
© 2022 by SLS, Society of Laparoscopic & Robotic Surgeons.
Figures
References
-
- Navarra G, Pozza E, Occhionorelli S, Carcoforo P, Donini I. Short note: one wound laparoscopic cholecystectomy. Br J Surg. 1997;84(5):695–695. - PubMed
-
- Ponsky TA, Diluciano J, Chwals W, Parry R, Boulanger S. Early experience with single port laparoscopic surgery in children. J Laparoendosc Adv Surg Tech A. 2009;19(4):551–553. - PubMed
-
- Saber AA, El-Ghazaly TH, Dewoolkar AV. Single-incision laparoscopic bariatric surgery: a comprehensive review. Surg Obes Relat Dis. 2010;6(5):575–582. - PubMed
-
- Chow AG, Purkayastha S, Zacharakis E, Paraskeva P. Single incision laparoscopic surgery for right hemicolectomy. Arch Surg. 2011;146(2):183–186. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources