

Clinical Features Differ Between Patients With Vertigo Attack Only and Weakness Attack Accompanying Vertigo Before Vertebrobasilar Stroke: A Retrospective Study
- PMID: 35968280
- PMCID: PMC9363826
- DOI: 10.3389/fneur.2022.928902
Clinical Features Differ Between Patients With Vertigo Attack Only and Weakness Attack Accompanying Vertigo Before Vertebrobasilar Stroke: A Retrospective Study
Abstract
Objective: To determine the different clinical features of patients with vertigo attacks alone and of those with weakness accompanying vertigo attacks before the vertebrobasilar ischemic stroke.
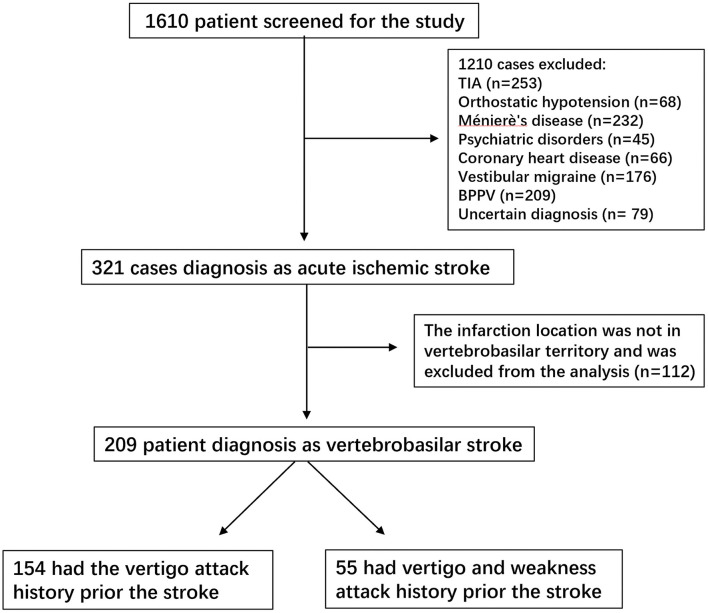
Methods: In this 4-year retrospective study, we manually screened the medical records of 209 patients, hospitalized with vertigo attack as the main complaint who were finally diagnosed with acute vertebrobasilar ischemic stroke. Patients were divided into two groups according to their symptoms: patients who only experienced vertigo attacks prior to the vertebrobasilar stroke (VO group) and patients who had both vertigo and weakness attacks (VW group) prior to the stroke. Clinical parameters, such as infarction site and volume, relative risk factors, ABCD2 score, and medical intervention, were compared between the two groups.
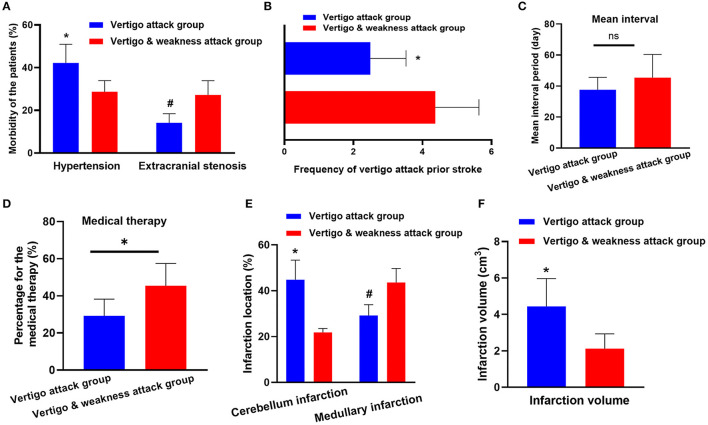
Results: The prevalence of hypertension was higher in the Vertigo attacks only (VO) group (42.2 vs. 29.0%, p < 0.05). The total cerebral infarction volume in the VO group was larger than the Vertigo and weakness attacks (VW) group (4.44 vs. 2.12 cm3, p < 0.05). Additionally, the cerebellum was more likely to be affected in the VO group. In contrast, patients in the VW group had higher carotid stenosis (14.2 vs. 27.2%, p < 0.05) and ABCD2 score (2.1 ± 1.2 vs. 3.6 ± 1.5, p = 0.02). The percentage of patients with medullary infarctions also increased in the VW group. Vertigo attack events occurred more frequently in the VW group (median 2.4 vs. 4.3, p < 0.04). We also found that the patients in the VW group were more likely to seek medical intervention after vertigo.
Conclusions: Clinical parameters, such as infarction location, relative risk factors, and ABCD2 score, differed between patients with vertigo symptoms with or without weakness attacks. These findings highlight the different clinical features of patients with vertigo attack only and those with weakness attacks accompanying vertigo prior to vertebrobasilar ischemic stroke.
Keywords: cerebral infarction; infarction; vertebrobasilar stroke; vertigo attack; weakness attack.
Copyright © 2022 Deng, Zhang, Zhang, Duan, Huang and Qiu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources