

Three-dimensional versus two-dimensional laparoscopic surgery for rectal cancer: better promote postoperative sexual and urinary function of a propensity-matched study
- PMID: 35968332
- PMCID: PMC9360212
Three-dimensional versus two-dimensional laparoscopic surgery for rectal cancer: better promote postoperative sexual and urinary function of a propensity-matched study
Abstract
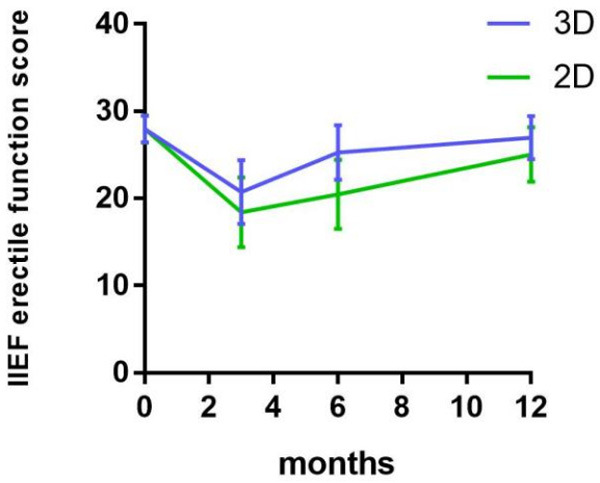
Laparoscopic total mesorectal excision (TME) with autonomic nerve preservation (ANP) is a common procedure for rectal cancer (RC), associated with a high prevalence of postoperative urogenital and anorectal dysfunctions. Compared to 2D laparoscopy, 3D laparoscopy provides better depth perception of the surgical field and hand-eye coordination to achieve better outcomes. We compared the performance of 2D and 3D laparoscopy on preserving urogenital and anorectal function in TME+ANP surgery for rectal cancer using propensity-score matching. Data were collected from consecutive male patients who underwent 3D or 2D laparoscopic TME+ANP for primary RC at our institution between March 2012 and December 2020. The primary outcome was sexual and urinary function 1 year after surgery. A total of 450 male patients were eligible. After 1:1 matching, 146 cases were included in each group for analysis. One year after surgery, the prevalence of sexual dysfunction (International Index of Erectile Function score <26) was 8.22% in the 3D laparoscopic group and 44.52% in the 2D laparoscopic group, respectively (P=0.000) and a significant difference in the incidence of urinary retention was observed (n=3 and 24, respectively (P=0.000)). Moreover, blood loss, operative time, duration of hospital stay, and the time to first flatus in the 3D laparoscopic group were significantly less than in the 2D laparoscopic group. In conclusion, 3D laparoscopic TME is associated with lower incidences of postoperative sexual and urinary dysfunction than 2D laparoscopic TME for rectal cancer in male patients.
Keywords: Rectal cancer; autonomic nerve preservation; laparoscopic; sexual and urinary function; total mesorectal excision.
AJCR Copyright © 2022.
Conflict of interest statement
None.
Figures
Similar articles
-
[Efficiency analysis on functional protection of nerve plane-oriented laparoscopic total mesorectal excision].Zhonghua Wei Chang Wai Ke Za Zhi. 2019 Dec 25;22(12):1144-1151. doi: 10.3760/cma.j.issn.1671-0274.2019.12.009. Zhonghua Wei Chang Wai Ke Za Zhi. 2019. PMID: 31874530 Chinese.
-
[Robotic versus laparoscopic total mesorectal excision with partial preservation of Denonvilliers fascia: a comparative study of short-term efficacy and urinary and erectile function].Zhonghua Wei Chang Wai Ke Za Zhi. 2021 Apr 25;24(4):327-334. doi: 10.3760/cma.j.cn.441530-20200724-00444. Zhonghua Wei Chang Wai Ke Za Zhi. 2021. PMID: 33878822 Chinese.
-
Laparoscopic pelvic autonomic nerve-preserving surgery for patients with lower rectal cancer after chemoradiation therapy.Ann Surg Oncol. 2007 Apr;14(4):1285-7. doi: 10.1245/s10434-006-9052-6. Ann Surg Oncol. 2007. PMID: 17235719 Clinical Trial.
-
Protective effect of laparoscopic functional total mesorectal excision on urinary and sexual functions in male patients with mid-low rectal cancer.Asian J Surg. 2023 Jan;46(1):236-243. doi: 10.1016/j.asjsur.2022.03.050. Epub 2022 Mar 29. Asian J Surg. 2023. PMID: 35361550
-
Total mesorectal excision for rectal cancer with emphasis on pelvic autonomic nerve preservation: Expert technical tips for robotic surgery.Surg Oncol. 2015 Sep;24(3):172-80. doi: 10.1016/j.suronc.2015.06.012. Epub 2015 Jun 17. Surg Oncol. 2015. PMID: 26141555 Review.
Cited by
-
The consequences of laparoscopic fascial space priority approach to lateral lymph node dissection on urinary and sexual functionality.Wideochir Inne Tech Maloinwazyjne. 2023 Dec;18(4):639-644. doi: 10.5114/wiitm.2023.130532. Epub 2023 Aug 18. Wideochir Inne Tech Maloinwazyjne. 2023. PMID: 38239575 Free PMC article.
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019;69:7–34. - PubMed
-
- Global Burden of Disease Cancer Collaboration. Fitzmaurice C, Allen C, Barber RM, Barregard L, Bhutta ZA, Brenner H, Dicker DJ, Chimed-Orchir O, Dandona R, Dandona L, Fleming T, Forouzanfar MH, Hancock J, Hay RJ, Hunter-Merrill R, Huynh C, Hosgood HD, Johnson CO, Jonas JB, Khubchandani J, Kumar GA, Kutz M, Lan Q, Larson HJ, Liang X, Lim SS, Lopez AD, MacIntyre MF, Marczak L, Marquez N, Mokdad AH, Pinho C, Pourmalek F, Salomon JA, Sanabria JR, Sandar L, Sartorius B, Schwartz SM, Shackelford KA, Shibuya K, Stanaway J, Steiner C, Sun J, Takahashi K, Vollset SE, Vos T, Wagner JA, Wang H, Westerman R, Zeeb H, Zoeckler L, Abd-Allah F, Ahmed MB, Alabed S, Alam NK, Aldhahri SF, Alem G, Alemayohu MA, Ali R, Al-Raddadi R, Amare A, Amoako Y, Artaman A, Asayesh H, Atnafu N, Awasthi A, Saleem HB, Barac A, Bedi N, Bensenor I, Berhane A, Bernabé E, Betsu B, Binagwaho A, Boneya D, Campos-Nonato I, Castañeda-Orjuela C, Catalá-López F, Chiang P, Chibueze C, Chitheer A, Choi JY, Cowie B, Damtew S, das Neves J, Dey S, Dharmaratne S, Dhillon P, Ding E, Driscoll T, Ekwueme D, Endries AY, Farvid M, Farzadfar F, Fernandes J, Fischer F, G/Hiwot TT, Gebru A, Gopalani S, Hailu A, Horino M, Horita N, Husseini A, Huybrechts I, Inoue M, Islami F, Jakovljevic M, James S, Javanbakht M, Jee SH, Kasaeian A, Kedir MS, Khader YS, Khang YH, Kim D, Leigh J, Linn S, Lunevicius R, El Razek HMA, Malekzadeh R, Malta DC, Marcenes W, Markos D, Melaku YA, Meles KG, Mendoza W, Mengiste DT, Meretoja TJ, Miller TR, Mohammad KA, Mohammadi A, Mohammed S, Moradi-Lakeh M, Nagel G, Nand D, Le Nguyen Q, Nolte S, Ogbo FA, Oladimeji KE, Oren E, Pa M, Park EK, Pereira DM, Plass D, Qorbani M, Radfar A, Rafay A, Rahman M, Rana SM, Søreide K, Satpathy M, Sawhney M, Sepanlou SG, Shaikh MA, She J, Shiue I, Shore HR, Shrime MG, So S, Soneji S, Stathopoulou V, Stroumpoulis K, Sufiyan MB, Sykes BL, Tabarés-Seisdedos R, Tadese F, Tedla BA, Tessema GA, Thakur JS, Tran BX, Ukwaja KN, Uzochukwu BSC, Vlassov VV, Weiderpass E, Wubshet Terefe M, Yebyo HG, Yimam HH, Yonemoto N, Younis MZ, Yu C, Zaidi Z, Zaki MES, Zenebe ZM, Murray CJL, Naghavi M. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 32 cancer groups, 1990 to 2015: a systematic analysis for the global burden of disease study. JAMA Oncol. 2017;3:524–548. - PMC - PubMed
-
- Miller KD, Siegel RL, Lin CC, Mariotto AB, Kramer JL, Rowland JH, Stein KD, Alteri R, Jemal A. Cancer treatment and survivorship statistics, 2016. CA Cancer J Clin. 2016;66:271–289. - PubMed
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209–249. - PubMed
LinkOut - more resources
Full Text Sources