

Machine learning-assisted prediction of pneumonia based on non-invasive measures
- PMID: 35968461
- PMCID: PMC9371749
- DOI: 10.3389/fpubh.2022.938801
Machine learning-assisted prediction of pneumonia based on non-invasive measures
Abstract
Background: Pneumonia is an infection of the lungs that is characterized by high morbidity and mortality. The use of machine learning systems to detect respiratory diseases via non-invasive measures such as physical and laboratory parameters is gaining momentum and has been proposed to decrease diagnostic uncertainty associated with bacterial pneumonia. Herein, this study conducted several experiments using eight machine learning models to predict pneumonia based on biomarkers, laboratory parameters, and physical features.
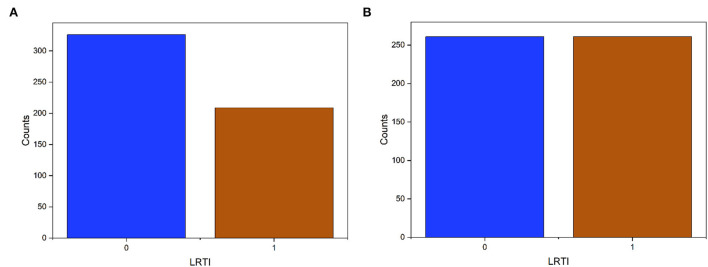
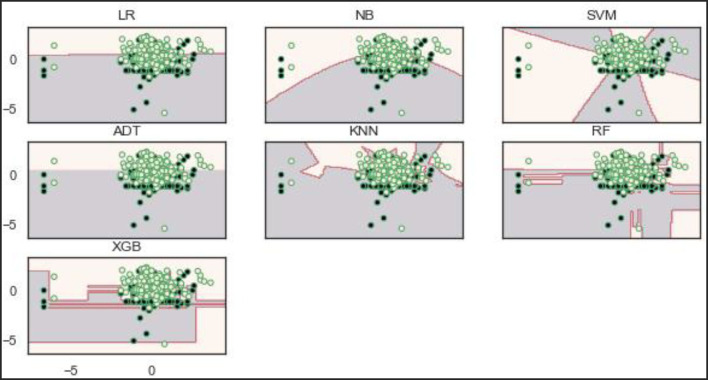
Methods: We perform machine-learning analysis on 535 different patients, each with 45 features. Data normalization to rescale all real-valued features was performed. Since it is a binary problem, we categorized each patient into one class at a time. We designed three experiments to evaluate the models: (1) feature selection techniques to select appropriate features for the models, (2) experiments on the imbalanced original dataset, and (3) experiments on the SMOTE data. We then compared eight machine learning models to evaluate their effectiveness in predicting pneumonia.
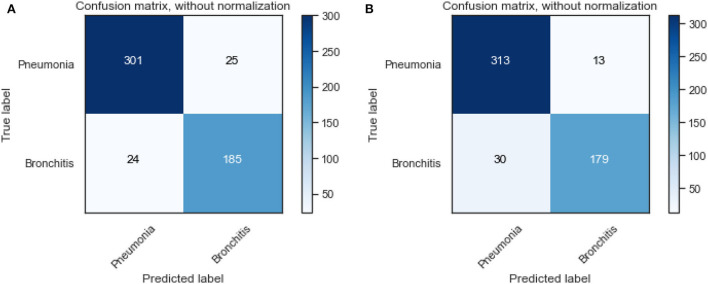
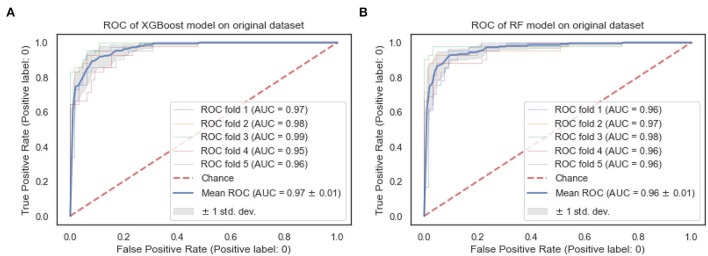
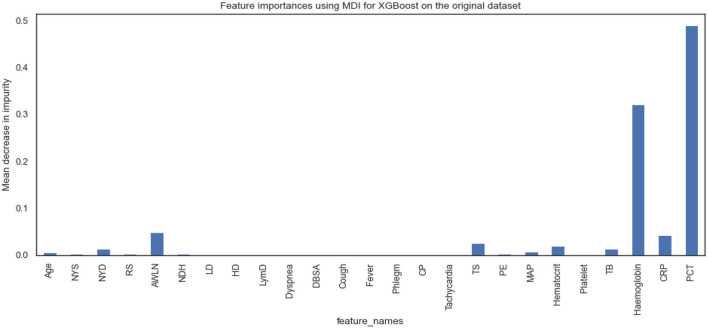
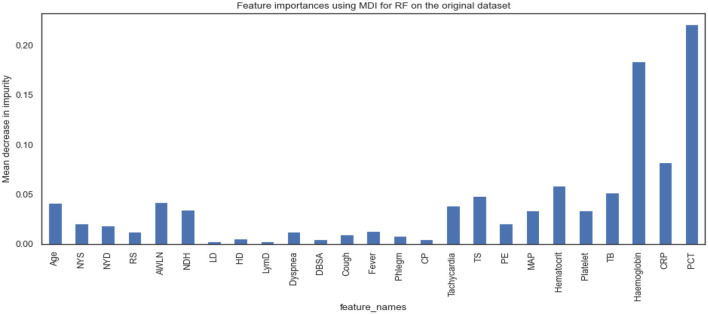
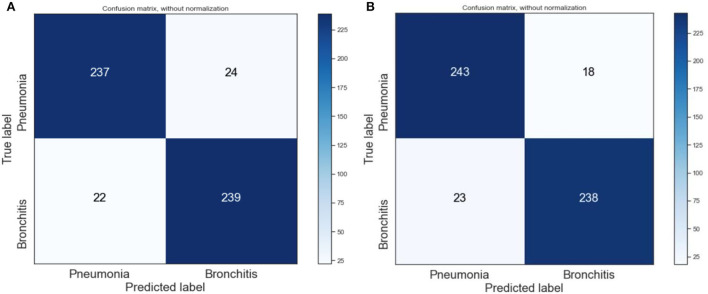
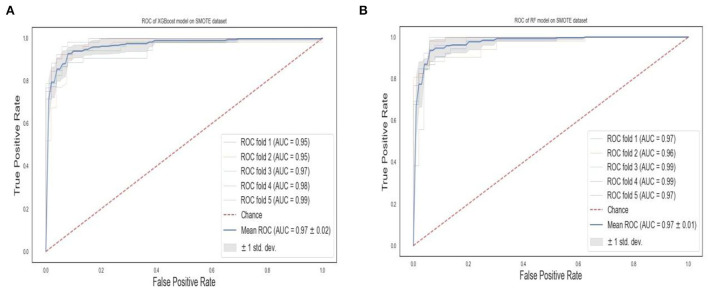
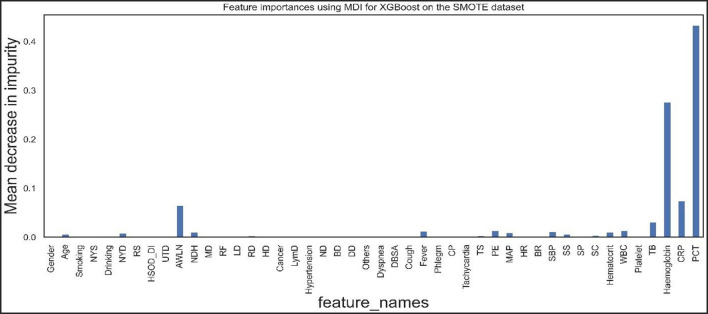
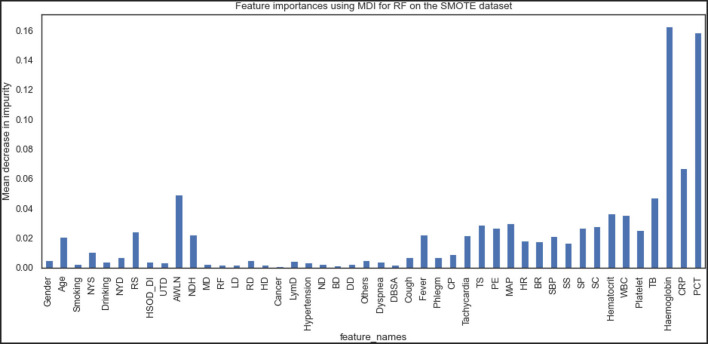
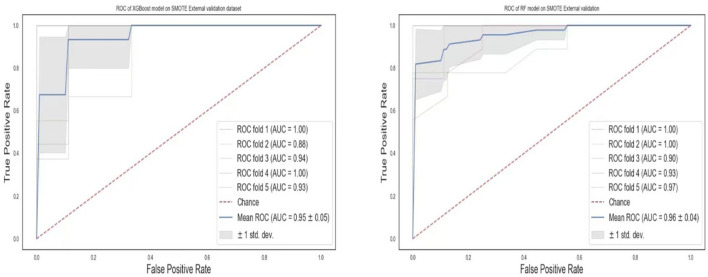
Results: Biomarkers such as C-reactive protein and procalcitonin demonstrated the most significant discriminating power. Ensemble machine learning models such as RF (accuracy = 92.0%, precision = 91.3%, recall = 96.0%, f1-Score = 93.6%) and XGBoost (accuracy = 90.8%, precision = 92.6%, recall = 92.3%, f1-score = 92.4%) achieved the highest performance accuracy on the original dataset with AUCs of 0.96 and 0.97, respectively. On the SMOTE dataset, RF and XGBoost achieved the highest prediction results with f1-scores of 92.0 and 91.2%, respectively. Also, AUC of 0.97 was achieved for both RF and XGBoost models.
Conclusions: Our models showed that in the diagnosis of pneumonia, individual clinical history, laboratory indicators, and symptoms do not have adequate discriminatory power. We can also conclude that the ensemble ML models performed better in this study.
Keywords: decision support system (DSS); electronic health records (EHR); machine learning; non-invasive measures; pneumonia.
Copyright © 2022 Effah, Miao, Drokow, Agboyibor, Qiao, Wu, Miao and Wang.
Conflict of interest statement
Author YaW was employed by Center of Health Management, General Hospital of Anyang Iron and Steel Group Co., Ltd. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- O'Brien KL, Baggett HC, Brooks WA, Feikin DR, Hammitt LL, Higdon MM, et al. Causes of severe pneumonia requiring hospital admission in children without HIV infection from Africa and Asia: the PERCH multi-country case-control study. Lancet. (2019) 394:757–79. 10.1016/S0140-6736(19)30721-4 - DOI - PMC - PubMed
-
- World Health Organization pneumonia vaccine trial investigator' group . Standardization of Interpretation of Chest Radiographs for the Diagnosis of Pneumonia in Children. (2001). p. 1–39.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials