

Evaluating the impact and cost-effectiveness of chlamydia management strategies in Hong Kong: A modeling study
- PMID: 35968473
- PMCID: PMC9363901
- DOI: 10.3389/fpubh.2022.932096
Evaluating the impact and cost-effectiveness of chlamydia management strategies in Hong Kong: A modeling study
Abstract
Objectives: To illustrate the epidemiologic and cost-effectiveness impact of shifting the focus from population-based screening toward a targeted management approach for genital chlamydia infection.
Design: Modeling study, implementing an individual-based, stochastic, dynamic network model.
Setting: Hong Kong.
Population: A hypothetical sample network of 10,000 people with a partnership distribution based on Hong Kong's sexually active population of reproductive age (age 18-49 years).
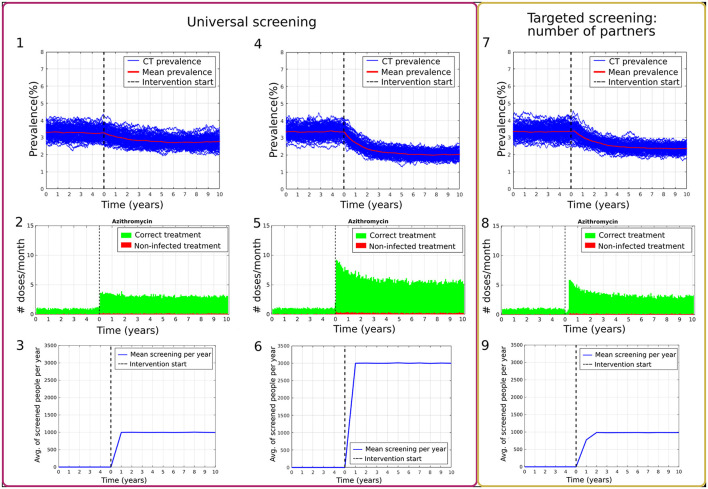
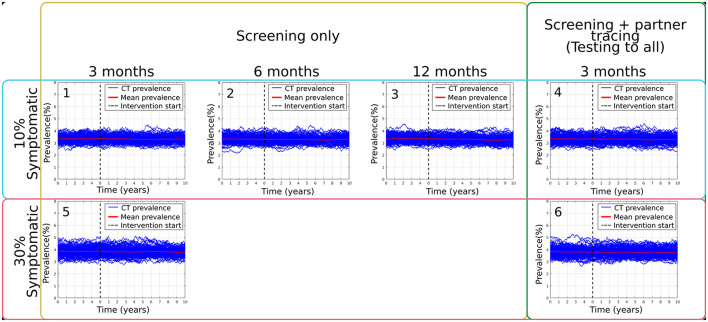
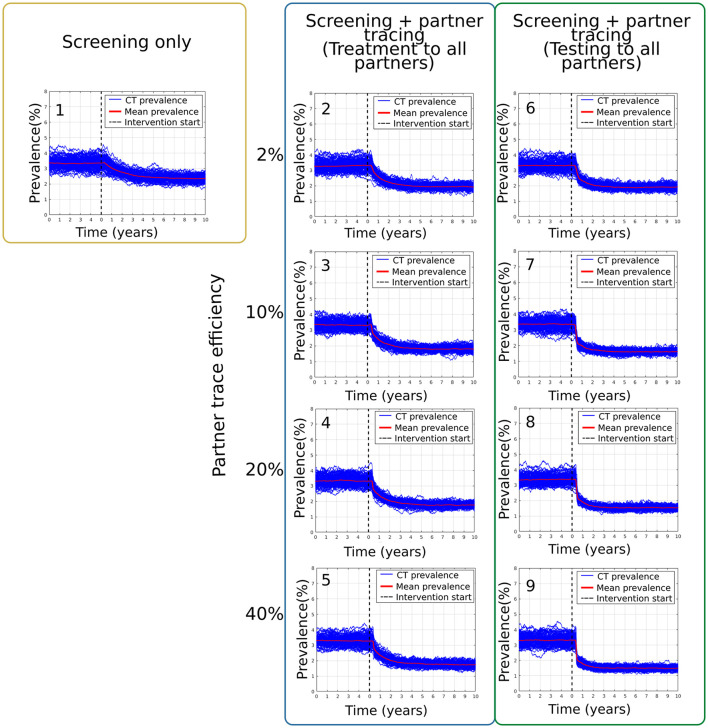
Interventions: In this study, we present several scenarios with different implementations of universal vs. targeted screening (based on partner numbers). We also explored the impact of (1) screening only, (2) screening plus expedited partner therapy, and (3) screening plus partner testing.
Primary outcome measures: Change of chlamydia prevalence before and after implementing the different strategies. The cost-effectiveness analysis reports total direct cost from a health provider perspective, the QALYs gained, and incremental cost-effectiveness ratios (ICER).
Results: In comparing the effects of universal screening only and targeted screening of the high-risk population, the mean prevalence during the 10th year of intervention was 2.75 ± 0.30% and 2.35 ± 0.21%, respectively (compared with 3.24 ± 0.30% and 3.35 ± 0.21% before the interventions, respectively). The addition of contact tracing to the latter targeted screening scenario reduces the mean prevalence during the 10th year of intervention to 1.48 ± 0.13% (compared with 3.31 ± 0.33% at baseline) in the best-case of testing before treatment and maximal contact-tracing effectiveness (40%). Overall, the most effective scenarios were those for which interventions focused on the high-risk population defined by the number of partners, with contact tracing included. The ICER for targeted screening with contact tracing at 20% and 40% efficiency was $4,634 and $7,219 per QALY gained, respectively (10-year time horizon). Expedited partner therapy did not significantly impact overall chlamydia prevalence and caused overtreatment.
Conclusions: Our study suggests that targeted screening with strengthened contact tracing efforts is the most cost-effective strategy to reduce the prevalence of chlamydia in Hong Kong.
Keywords: chlamydia; cost-effectiveness; dynamic network models; economic evaluation; stochastic model.
Copyright © 2022 Montes-Olivas, Ozten, Homer, Turner, Fairley, Hocking, Tse, Verschueren van Rees, Wong and Ong.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Effectiveness and cost-effectiveness of traditional and new partner notification technologies for curable sexually transmitted infections: observational study, systematic reviews and mathematical modelling.Health Technol Assess. 2014 Jan;18(2):1-100, vii-viii. doi: 10.3310/hta18020. Health Technol Assess. 2014. PMID: 24411488 Free PMC article. Review.
-
Impact and cost-effectiveness of chlamydia testing in Scotland: a mathematical modelling study.Theor Biol Med Model. 2015 Jan 15;12:2. doi: 10.1186/1742-4682-12-2. Theor Biol Med Model. 2015. PMID: 25588390 Free PMC article.
-
Costs, Health Benefits, and Cost-Effectiveness of Chlamydia Screening and Partner Notification in the United States, 2000-2019: A Mathematical Modeling Analysis.Sex Transm Dis. 2023 Jun 1;50(6):351-358. doi: 10.1097/OLQ.0000000000001786. Epub 2023 Feb 20. Sex Transm Dis. 2023. PMID: 36804917 Free PMC article.
-
Cost-effectiveness of two screening strategies for Chlamydia trachomatis and Neisseria gonorrhoeae as part of the PrEP programme in the Netherlands: a modelling study.Sex Transm Infect. 2021 Dec;97(8):607-612. doi: 10.1136/sextrans-2020-054741. Epub 2021 Jan 11. Sex Transm Infect. 2021. PMID: 33431605
-
Epidemiological, social, diagnostic and economic evaluation of population screening for genital chlamydial infection.Health Technol Assess. 2007 Mar;11(8):iii-iv, ix-xii, 1-165. doi: 10.3310/hta11080. Health Technol Assess. 2007. PMID: 17311735 Review.
References
-
- Worboys M. Wellcome Trust–Funded Monographs and Book Chapters. Chlamydia: A Disease without a History. In: Szreter S. editor. The Hidden Affliction: Sexually Transmitted Infections and Infertility in History. Rochester (NY): University of Rochester Press Copyright 2019 by the Editors and Contributors. (2019).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical