

The Impact of Hip Fracture on Geriatric Care and Mortality Among Older Swedes: Mapping Care Trajectories and Their Determinants
- PMID: 35968686
- PMCID: PMC9825727
- DOI: 10.1093/aje/kwac149
The Impact of Hip Fracture on Geriatric Care and Mortality Among Older Swedes: Mapping Care Trajectories and Their Determinants
Abstract
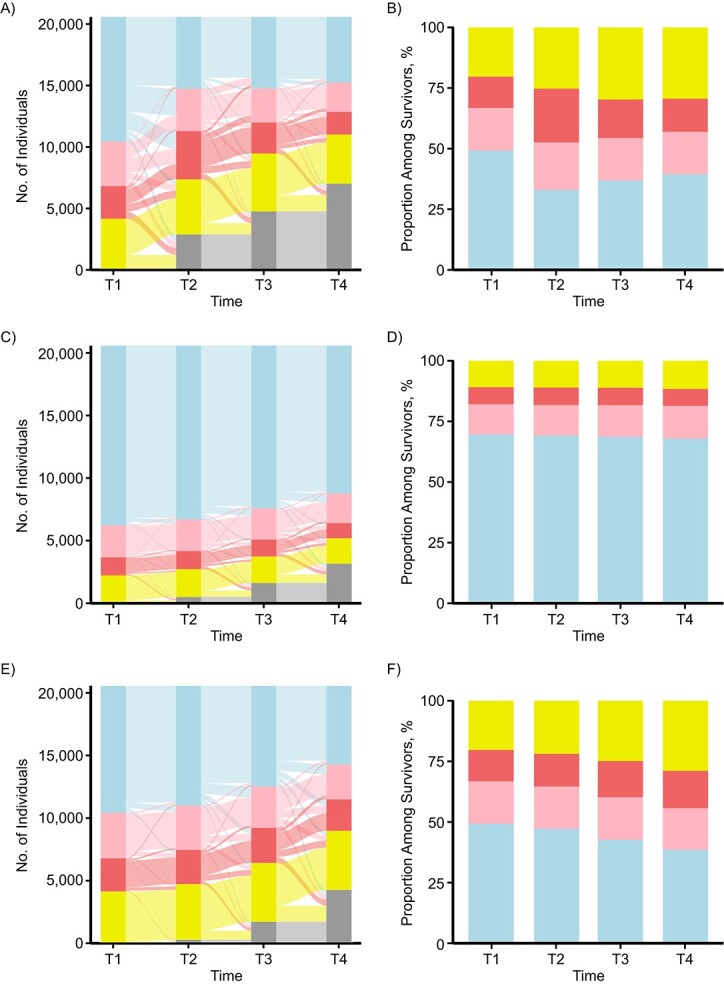
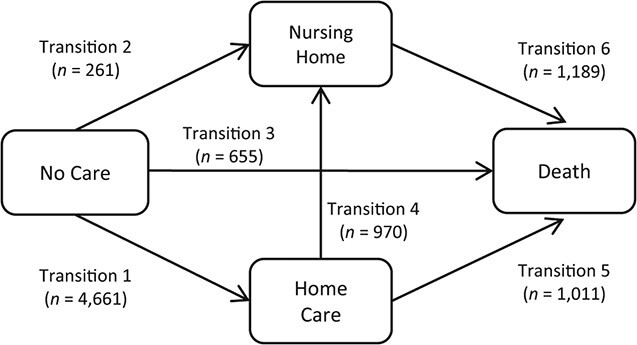
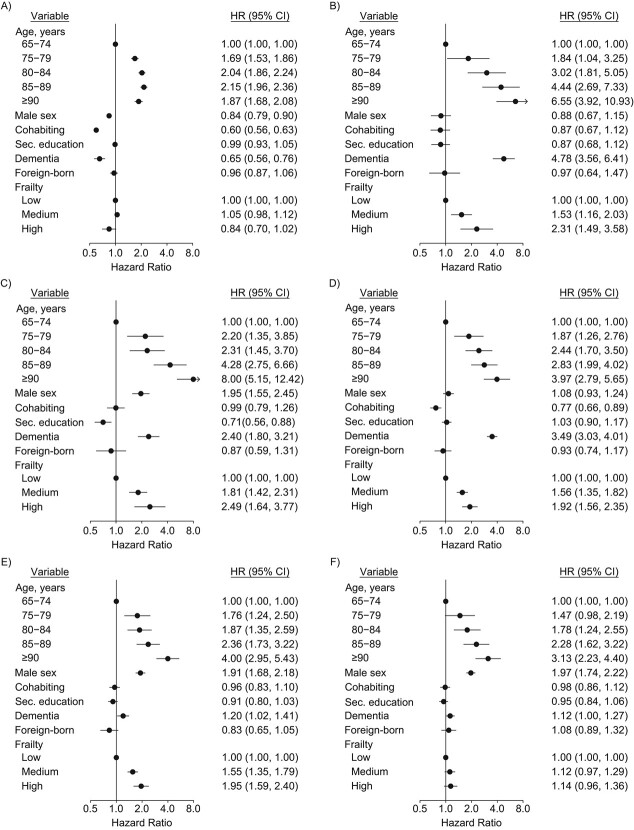
In this study, we examined the impact of hip fractures on trajectories of home care, nursing home residence, and mortality among individuals aged 65 years or more and explored the impacts of living arrangements, cohabitation, frailty, and socioeconomic position on these trajectories. Based on a linkage of nationwide Swedish population registers, our study included 20,573 individuals with first hip fracture in 2014-2015. Care trajectories during the 2 years following the fracture were visualized and compared with those of 2 hip-fracture-free control groups drawn from the general population: age- and sex-matched controls and health-matched controls identified through propensity score matching. Multistate modeling was employed to identify sociodemographic and health-related factors associated with care trajectories among hip fracture patients. We found that hip fracture patients already had worse health than the general population before their fracture. However, when controlling for prefracture health, hip fractures still had a considerable impact on use of elder-care services and mortality. Comparisons with the health-matched controls suggest that hip fractures have an immediate, yet short-term, impact on care trajectories. Long-term care needs are largely attributable to poorer health profiles independent of the fracture itself. This emphasizes the importance of adequate comparison groups when examining the consequences of diseases which are often accompanied by other underlying health problems.
Keywords: Sweden; aging; elder care; hip fracture; home care; nursing homes; osteoporosis; registers.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Johns Hopkins Bloomberg School of Public Health.
Figures
References
-
- Peeters CMM, Visser E, Van de Ree CLP, et al. Quality of life after hip fracture in the elderly: a systematic literature review. Injury. 2016;47(7):1369–1382. - PubMed
-
- Bertram M, Norman R, Kemp L, et al. Review of the long-term disability associated with hip fractures. Inj Prev. 2011;17(6):365–370. - PubMed
-
- Abrahamsen B, Staa T, Ariely R, et al. Excess mortality following hip fracture: a systematic epidemiological review. Osteoporos Int. 2009;20(10):1633–1650. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
