

Implementation and outcomes of a clinician-directed intervention to improve antibiotic prescribing for acute respiratory tract infections within the Veterans' Affairs Healthcare System
- PMID: 35968847
- PMCID: PMC10882581
- DOI: 10.1017/ice.2022.182
Implementation and outcomes of a clinician-directed intervention to improve antibiotic prescribing for acute respiratory tract infections within the Veterans' Affairs Healthcare System
Abstract
Objective: To determine whether a clinician-directed acute respiratory tract infection (ARI) intervention was associated with improved antibiotic prescribing and patient outcomes across a large US healthcare system.
Design: Multicenter retrospective quasi-experimental analysis of outpatient visits with a diagnosis of uncomplicated ARI over a 7-year period.
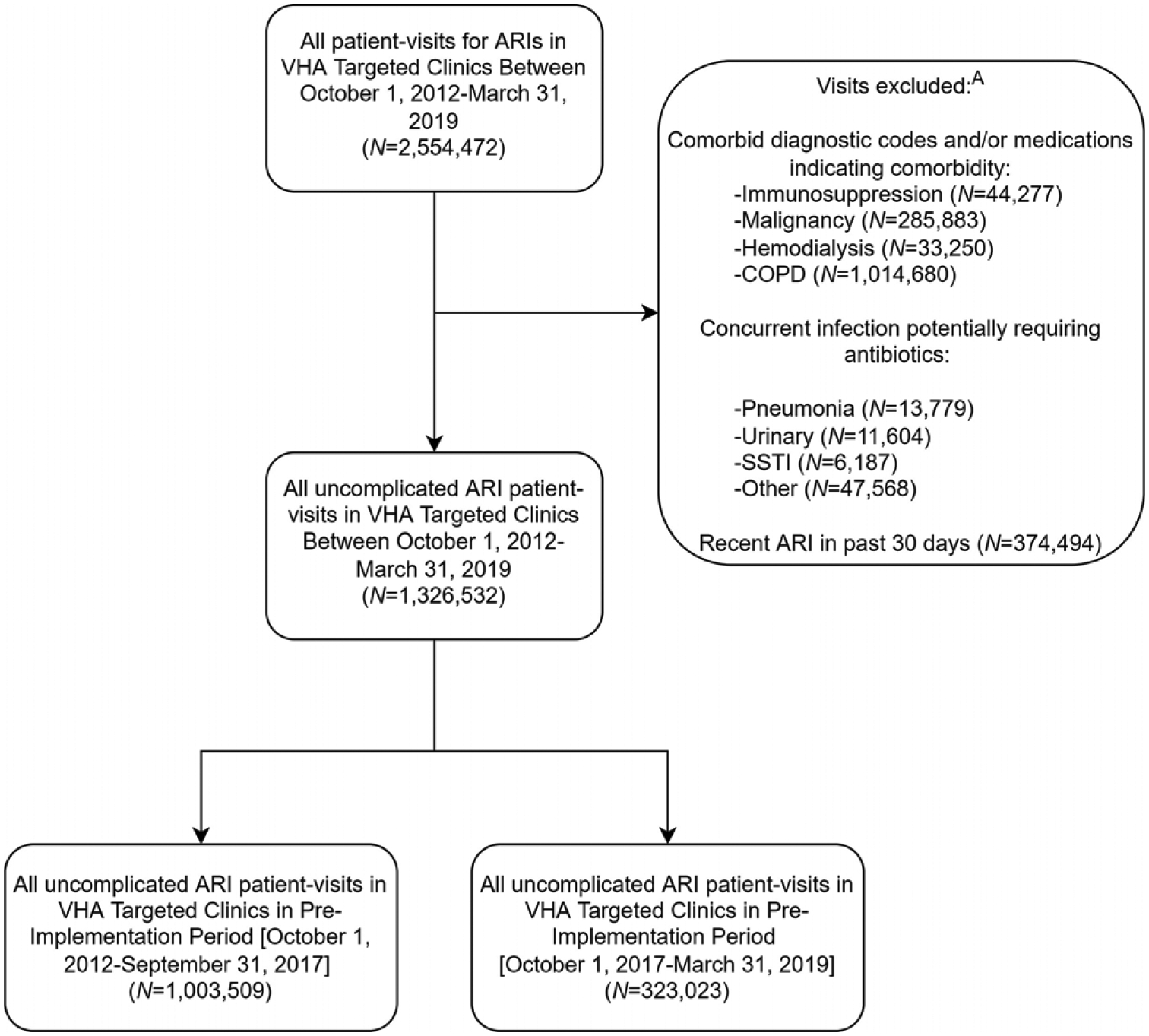
Participants: Outpatients with ARI diagnoses: sinusitis, pharyngitis, bronchitis, and unspecified upper respiratory tract infection (URI-NOS). Outpatients with concurrent infection or select comorbid conditions were excluded.
Intervention(s): Audit and feedback with peer comparison of antibiotic prescribing rates and academic detailing of clinicians with frequent ARI visits. Antimicrobial stewards and academic detailing personnel delivered the intervention; facility and clinician participation were voluntary.
Measure(s): We calculated the probability to receive antibiotics for an ARI before and after implementation. Secondary outcomes included probability for a return clinic visits or infection-related hospitalization, before and after implementation. Intervention effects were assessed with logistic generalized estimating equation models. Facility participation was tracked, and results were stratified by quartile of facility intervention intensity.
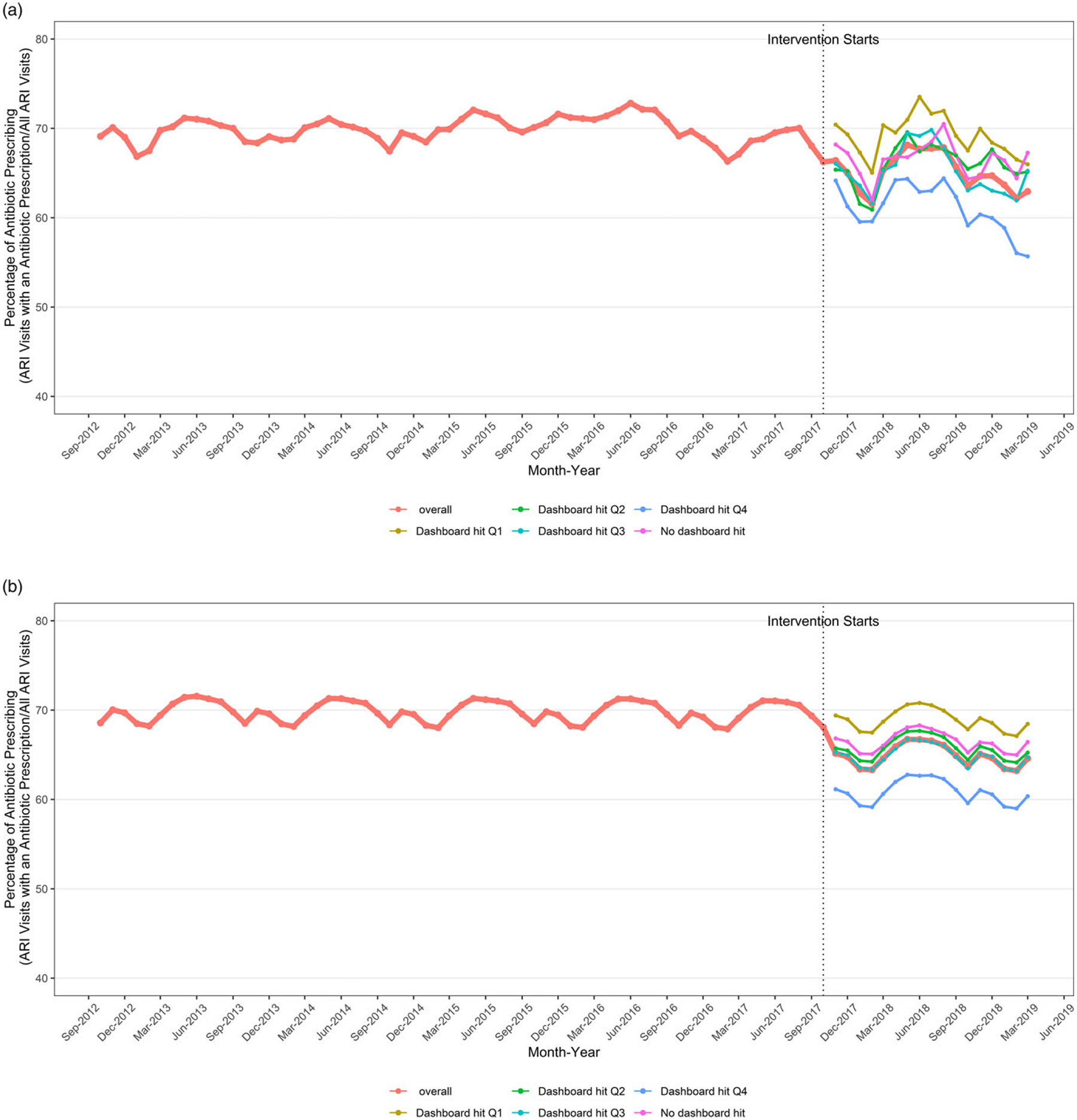
Results: We reviewed 1,003,509 and 323,023 uncomplicated ARI visits before and after the implementation of the intervention, respectively. The probability to receive antibiotics for ARI decreased after implementation (odds ratio [OR], 0.82; 95% confidence interval [CI], 0.78-0.86). Facilities with the highest quartile of intervention intensity demonstrated larger reductions in antibiotic prescribing (OR, 0.69; 95% CI, 0.59-0.80) compared to nonparticipating facilities (OR, 0.89; 95% CI, 0.73-1.09). Return visits (OR, 1.00; 95% CI, 0.94-1.07) and infection-related hospitalizations (OR, 1.21; 95% CI, 0.92-1.59) were not different before and after implementation within facilities that performed intensive implementation.
Conclusions: Implementation of a nationwide ARI management intervention (ie, audit and feedback with academic detailing) was associated with improved ARI management in an intervention intensity-dependent manner. No impact on ARI-related clinical outcomes was observed.
Conflict of interest statement
Figures
Similar articles
-
Evaluation of uncomplicated acute respiratory tract infection management in veterans: A national utilization review.Infect Control Hosp Epidemiol. 2019 Apr;40(4):438-446. doi: 10.1017/ice.2019.16. Infect Control Hosp Epidemiol. 2019. PMID: 30973130
-
Impact of Implementation of the Core Elements of Outpatient Antibiotic Stewardship Within Veterans Health Administration Emergency Departments and Primary Care Clinics on Antibiotic Prescribing and Patient Outcomes.Clin Infect Dis. 2021 Sep 7;73(5):e1126-e1134. doi: 10.1093/cid/ciaa1831. Clin Infect Dis. 2021. PMID: 33289028
-
Behavioral interventions to reduce inappropriate antibiotic prescribing: a randomized pilot trial.BMC Infect Dis. 2016 Aug 5;16:373. doi: 10.1186/s12879-016-1715-8. BMC Infect Dis. 2016. PMID: 27495917 Free PMC article. Clinical Trial.
-
Antibiotic prescribing for acute respiratory infection and subsequent outpatient and hospital utilization in veterans with spinal cord injury and disorder.PM R. 2010 Feb;2(2):101-9. doi: 10.1016/j.pmrj.2009.11.002. Epub 2010 Feb 1. PM R. 2010. PMID: 20117971
-
Variation in Outpatient Antibiotic Prescribing for Acute Respiratory Infections in the Veteran Population: A Cross-sectional Study.Ann Intern Med. 2015 Jul 21;163(2):73-80. doi: 10.7326/M14-1933. Ann Intern Med. 2015. PMID: 26192562
Cited by
-
Antimicrobial stewardship strategy implementation and impact in acute care spinal cord injury and disorder units.J Spinal Cord Med. 2025 Jan;48(1):112-128. doi: 10.1080/10790268.2023.2277963. Epub 2023 Nov 20. J Spinal Cord Med. 2025. PMID: 37982811 Free PMC article.
-
Look-Back and Look-Forward Durations and the Apparent Appropriateness of Ambulatory Antibiotic Prescribing.Antibiotics (Basel). 2022 Nov 4;11(11):1554. doi: 10.3390/antibiotics11111554. Antibiotics (Basel). 2022. PMID: 36358209 Free PMC article.
-
Feasibility of a Low-Intensity Intervention to Influence Antibiotic Prescribing Rates Use in Outpatient Settings: A Cluster Randomized Controlled Clinical Trial.Open Forum Infect Dis. 2024 Dec 16;12(1):ofae725. doi: 10.1093/ofid/ofae725. eCollection 2025 Jan. Open Forum Infect Dis. 2024. PMID: 39758744 Free PMC article. Clinical Trial.
-
Quality improvement initiative to reduce URI-associated antibiotic prescriptions among adult primary care providers.BMJ Open Qual. 2024 Aug 9;13(3):e002811. doi: 10.1136/bmjoq-2024-002811. BMJ Open Qual. 2024. PMID: 39122444 Free PMC article.
References
-
- Fleming-Dutra KE, Hersh AL, Shapiro DJ, et al. Prevalence of inappropriate antibiotic prescriptions among US ambulatory care visits, 2010–2011. JAMA 2016;315:1864–1873. - PubMed
-
- Jones BE, Sauer B, Jones MM, et al. Variation in outpatient antibiotic prescribing for acute respiratory infections in the veteran population: a cross-sectional study. Ann Intern Med 2015;163:73–80. - PubMed
-
- Bohan JG, Madaras-Kelly K, Pontefract B, et al. ARI Management Improvement Group. Evaluation of uncomplicated acute respiratory tract infection management in veterans: a national utilization review. Infect Control Hosp Epidemiol 2019;40:438–446. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
