

The Use of Death Certificate Data to Characterize Mortality Associated With Respiratory Syncytial Virus, Unspecified Bronchiolitis, and Influenza in the United States, 1999-2018
- PMID: 35968872
- PMCID: PMC9377031
- DOI: 10.1093/infdis/jiac187
The Use of Death Certificate Data to Characterize Mortality Associated With Respiratory Syncytial Virus, Unspecified Bronchiolitis, and Influenza in the United States, 1999-2018
Abstract
Background: Death certificate data can improve our understanding of the mortality burden associated with respiratory syncytial virus (RSV) and influenza.
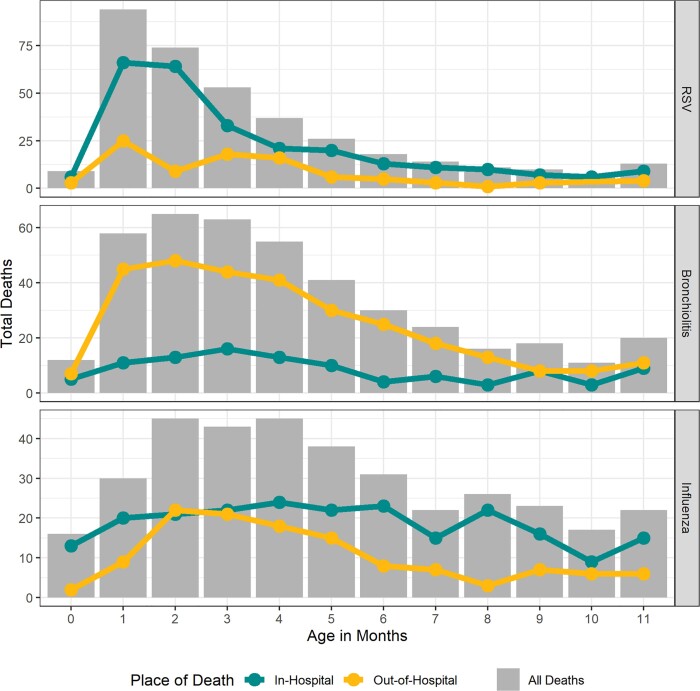
Methods: We used International Classification of Diseases, Tenth Revision codes listed on death certificates to characterize deaths from 1999 to 2018 as RSV, influenza, and unspecified bronchiolitis. We described the distribution of each cause of death by age, sex, race/ethnicity, place of death, and contributing causes of death.
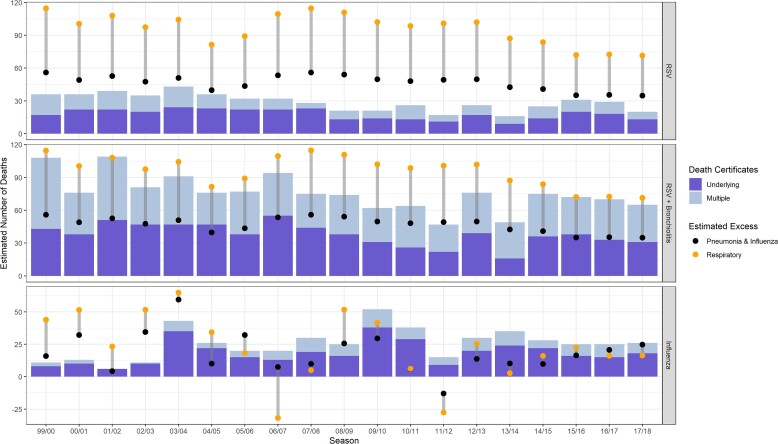
Results: Over the 20-year study period, RSV, bronchiolitis, and influenza were listed as the underlying causes of death on 932, 1046, and 52 293 death certificates, respectively. Children <1 year of age accounted for 39% of RSV and bronchiolitis deaths, while 72% of influenza deaths were in adults ≥65 years. Children <1 year were more likely to die outside of the hospital from RSV, bronchiolitis, or influenza compared to all causes (P < .01), and black infants had the highest mortality rate for all 3 causes. Most infants dying from RSV did not have a high-risk condition listed on the death certificate. Death certificates captured 20%-60% of estimated excess RSV-attributable mortality in infants and <1% in seniors.
Conclusions: Thorough reporting on death certificates is an important public health goal, especially as new therapeutics become available. Infants had higher odds of dying out of hospital from respiratory pathogens compared to other causes, and race/ethnicity alone did not explain this disparity.
Keywords: RSV; bronchiolitis; death certificates; excess mortality; infant mortality; influenza.
© The Author(s) 2022. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. C. L. H. received contract-based hourly fees from sanofi pasteur - Sanofi. S. S. C. is an employee of sanofi pasteur - Sanofi and may hold shares and/or stock options in the company. C. V. reports no potential conflicts of interest. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures

References
-
- Falsey AR, Hennessey PA, Formica MA, Cox C, Walsh EE. Respiratory syncytial virus infection in elderly and high-risk adults. N Engl J Med 2005; 352:1749–59. - PubMed
-
- Branche AR, Saiman L, Walsh EE, et al. Incidence of respiratory syncytial virus infection among hospitalized adults, 2017–2020. Clin Infect Dis 2022; 74:1004–11. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
