

Cost of Respiratory Syncytial Virus Infections in US Infants: Systematic Literature Review and Analysis
- PMID: 35968875
- PMCID: PMC9377037
- DOI: 10.1093/infdis/jiac172
Cost of Respiratory Syncytial Virus Infections in US Infants: Systematic Literature Review and Analysis
Abstract
Background: Limited data are available on the economic costs of respiratory syncytial virus (RSV) infections among infants and young children in the United States.
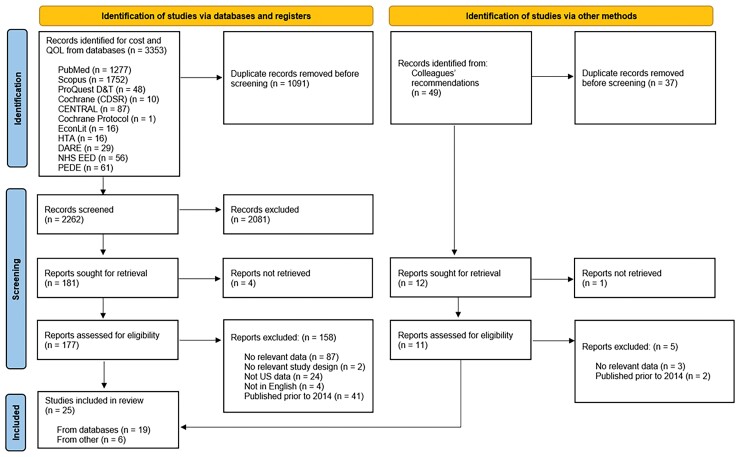
Methods: We performed a systematic literature review of 10 key databases to identify studies published between 1 January 2014 and 2 August 2021 that reported RSV-related costs in US children aged 0-59 months. Costs were extracted and a systematic analysis was performed.
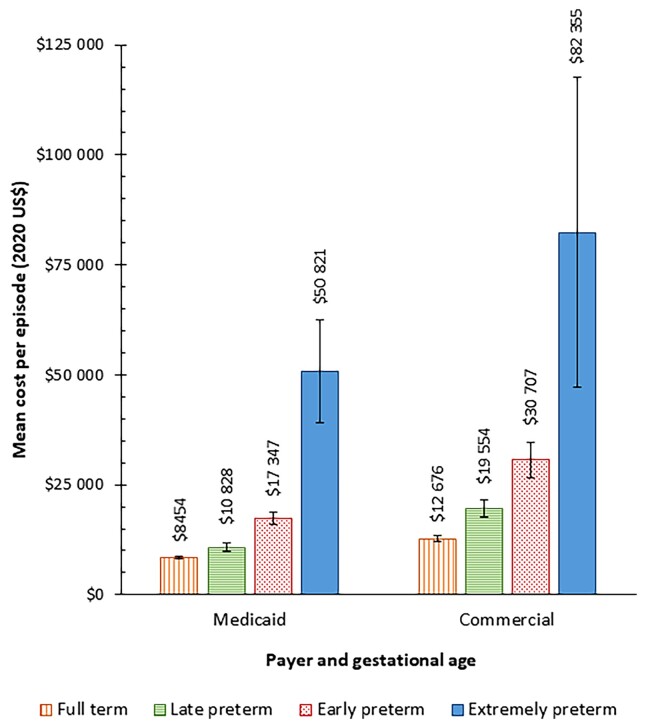
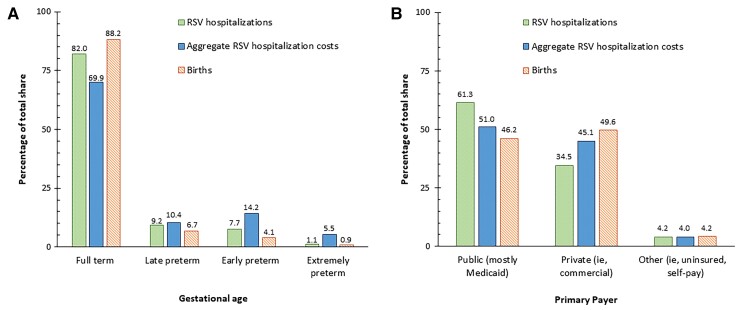
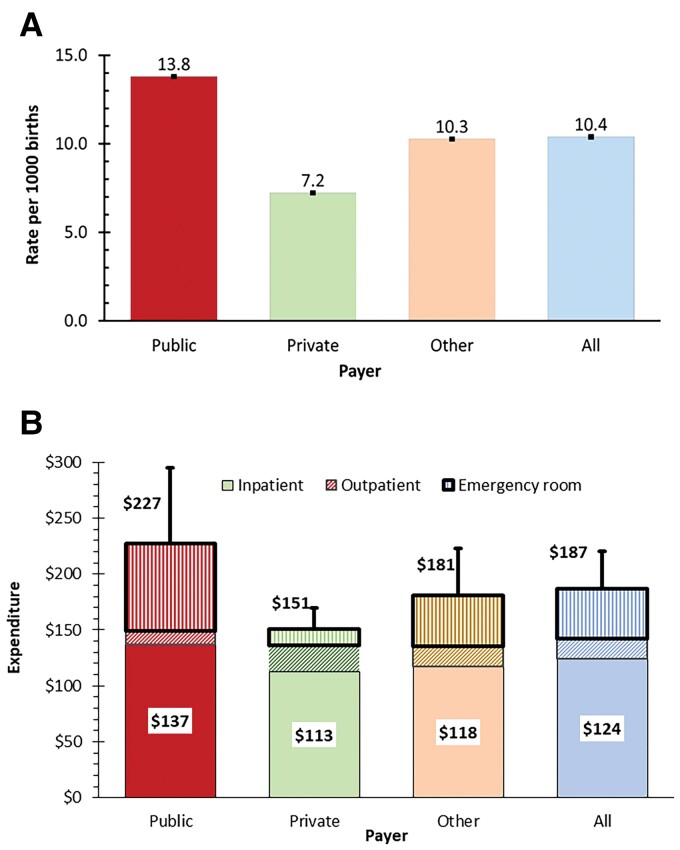
Results: Seventeen studies were included. Although an RSV hospitalization (RSVH) of an extremely premature infant costs 5.6 times that of a full-term infant ($10 214), full-term infants accounted for 82% of RSVHs and 70% of RSVH costs. Medicaid-insured infants were 91% more likely than commercially insured infants to be hospitalized for RSV treatment in their first year of life. Medicaid financed 61% of infant RSVHs. Paying 32% less per hospitalization than commercial insurance, Medicaid paid 51% of infant RSVH costs. Infants' RSV treatment costs $709.6 million annually, representing $187 per overall birth and $227 per publicly funded birth.
Conclusions: Public sources pay for more than half of infants' RSV medical costs, constituting the highest rate of RSVHs and the highest expenditure per birth. Full-term infants are the predominant source of infant RSVHs and costs.
Keywords: Medicaid; RSV; economic cost; gestational age; hospitalization; infant; premature; respiratory syncytial virus; systematic analysis; systematic literature review.
© The Author(s) 2022. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. D. M. B., K. R. R., D. H., R. M. G., Y. H.-R., and E. L. G. were supported in part under an agreement between Sanofi and Brandeis University, but none received any direct funding nor in-kind support from the sponsors. C. B. N. is an employee of Sanofi and may hold shares and/or stock options in the company. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- Walsh EE, Hall Breese C. Respiratory syncytial virus (RSV). In: Bennett JE, Dolin R, Blaser MJ, eds. Mandell D and Bennett’s principles and practice of infectious diseases. 8th ed.2015:1948–60.e1943.
-
- Haddadin Z, Rankin DA, Lipworth L, et al. Respiratory virus surveillance in infants across different clinical settings. J Pediat 2021; 234:164–71. - PubMed
-
- Lively JY, Curns AT, Weinberg GA, et al. Respiratory syncytial virus-associated outpatient visits among children younger than 24 months. J Pediatric Infect Dis Soc 2019; 8:284–6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
