

Respiratory Syncytial Virus Burden and Healthcare Utilization in United States Infants <1 Year of Age: Study of Nationally Representative Databases, 2011-2019
- PMID: 35968879
- PMCID: PMC9377028
- DOI: 10.1093/infdis/jiac155
Respiratory Syncytial Virus Burden and Healthcare Utilization in United States Infants <1 Year of Age: Study of Nationally Representative Databases, 2011-2019
Abstract
Background: Respiratory syncytial virus (RSV) is the leading cause of hospitalizations in United States infants aged <1 year, but research has focused on select populations.
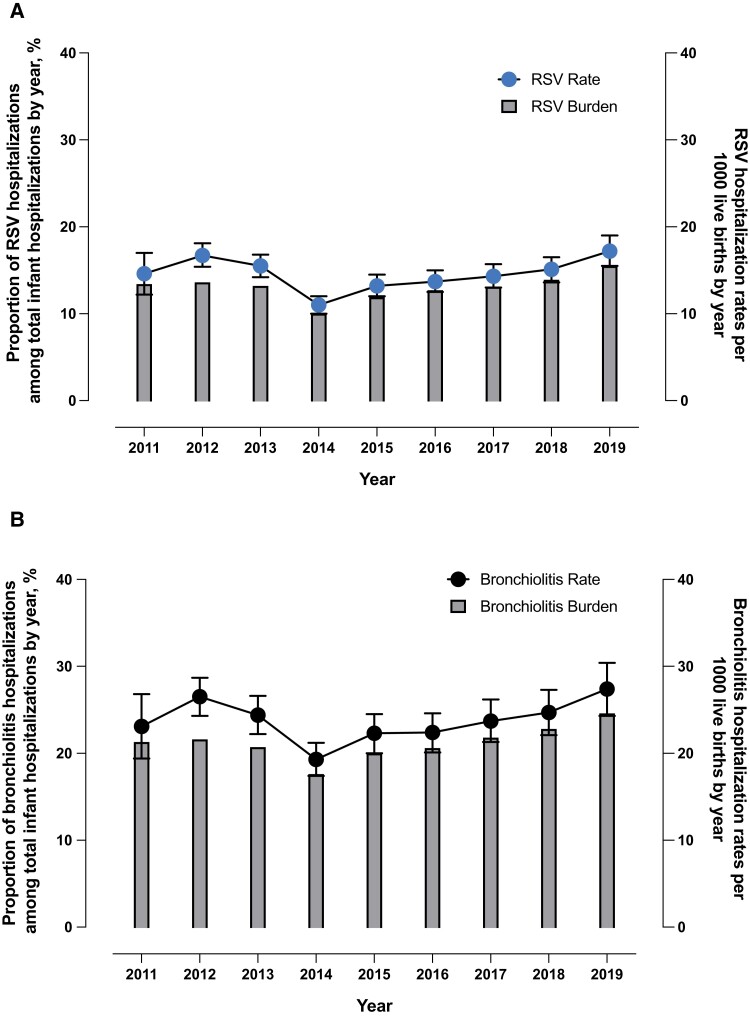
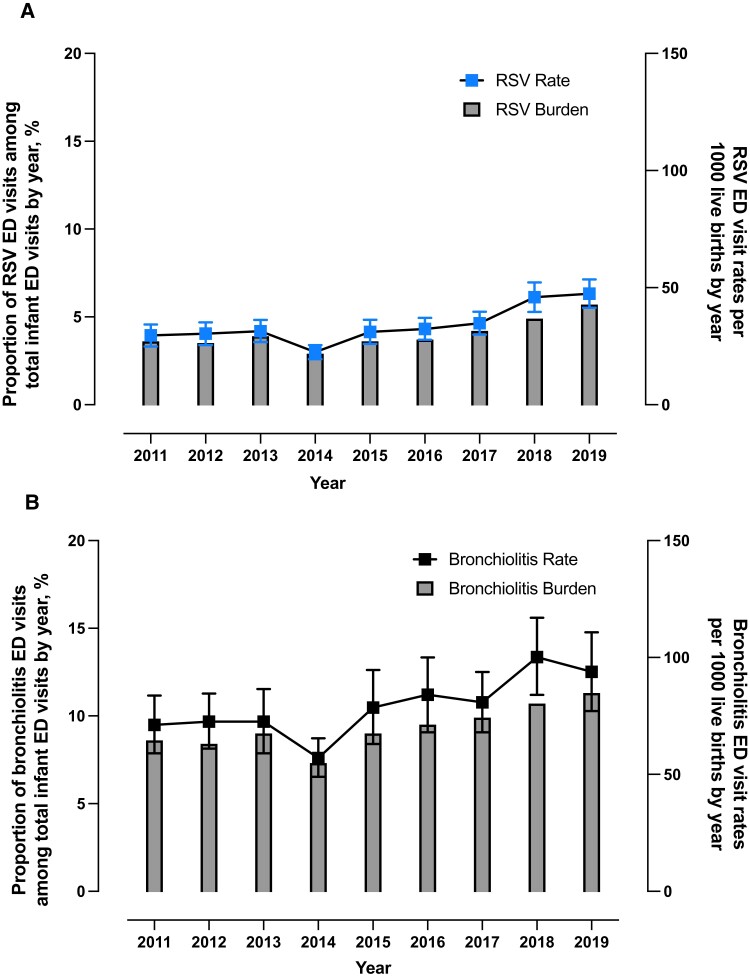
Methods: National (Nationwide) Inpatient Sample and National Emergency Department (ED) Sample data (2011-2019) were used to report RSV hospitalization (RSVH), bronchiolitis hospitalization (BH), and ED visit counts, percentage of total hospitalizations/visits, and rates per 1000 live births along with inpatient mortality, mechanical ventilation (MV), and total charges (2020 US dollars).
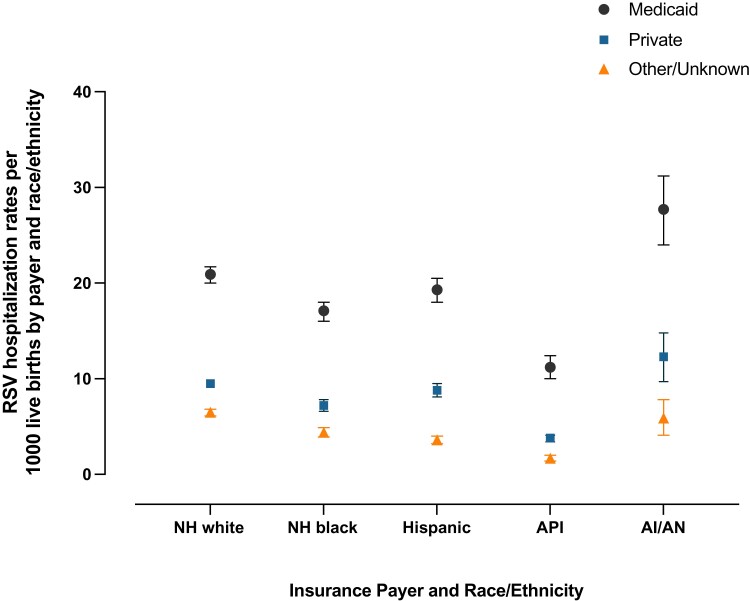
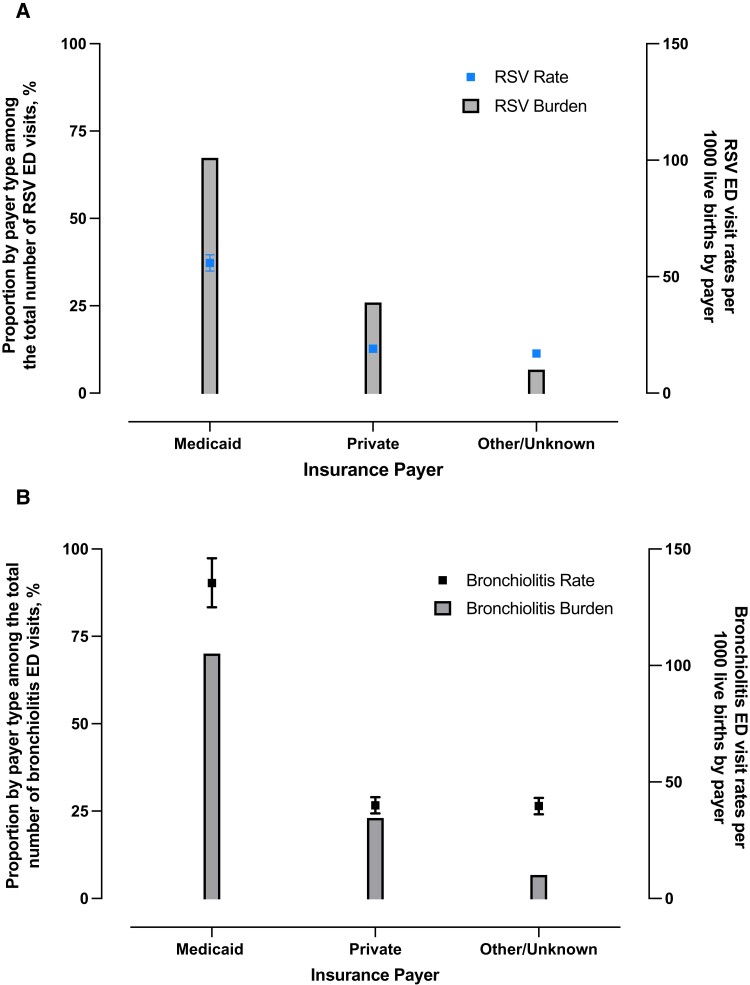
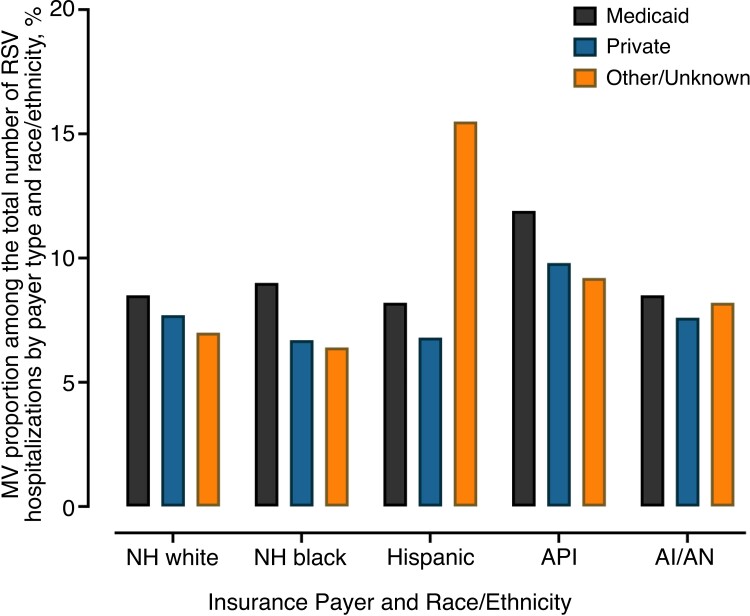
Results: Average annual RSVH and RSV ED visits were 56 927 (range, 43 845-66 155) and 131 999 (range, 89 809-177 680), respectively. RSVH rates remained constant over time (P = .5), whereas ED visit rates increased (P = .004). From 2011 through 2019, Medicaid infants had the highest average rates (RSVH: 22.3 [95% confidence interval {CI}, 21.5-23.1] per 1000; ED visits: 55.9 [95% CI, 52.4-59.4] per 1000) compared to infants with private or other/unknown insurance (RSVH: P < .0001; ED visits: P < .0001). From 2011 through 2019, for all races and ethnicities, Medicaid infants had higher average RSVH rates (up to 7 times) compared to infants with private or other/unknown insurance. RSVH mortality remained constant over time (P = .8), whereas MV use (2019: 13% of RSVH, P < .0001) and mean charge during hospitalization (2019: $21 513, P < .0001) increased. Bronchiolitis patterns were similar.
Conclusions: This study highlights the importance of ensuring access to RSV preventive measures for all infants.
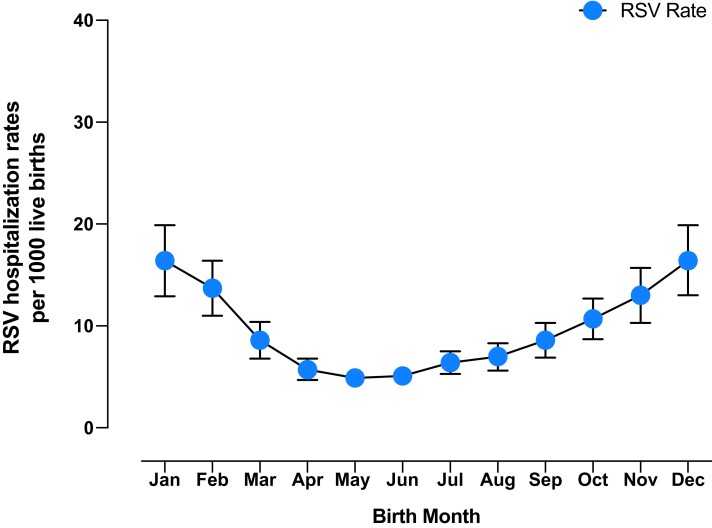
Keywords: Medicaid; RSV; RSV hospitalizations; birth month; bronchiolitis hospitalizations; emergency department; infants; respiratory syncytial virus.
© The Author(s) 2022. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. EpidStrategies received a grant from Sanofi for this research. M. S., N. M., X. J., H. R., L. C. B., and J. P. F. are employees of EpidStrategies. C. B. N. is an employee of Sanofi and may hold shares and/or stock options in the company. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures

References
-
- Leader S, Kohlhase K. Recent trends in severe respiratory syncytial virus (RSV) among US infants, 1997 to 2000. J Pediatr 2003; 143:S127–32. - PubMed
-
- Holman RC, Curns AT, Cheek JE, et al. Respiratory syncytial virus hospitalizations among American Indian and Alaska Native infants and the general United States infant population. Pediatrics 2004; 114:e437–44. - PubMed
-
- Yorita KL, Holman RC, Sejvar JJ, Steiner CA, Schonberger LB. Infectious disease hospitalizations among infants in the United States. Pediatrics 2008; 121:244–52. - PubMed
-
- Ledbetter J, Brannman L, Wade SW, Gonzales T, Kong AM. Healthcare resource utilization and costs in the 12 months following hospitalization for respiratory syncytial virus or unspecified bronchiolitis among infants. J Med Econ 2020; 23:139–47. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
