

Actionable Factors Fostering Health Value Generation and Scalability of Prehabilitation: A Prospective Cohort Study
- PMID: 35968894
- PMCID: PMC10321511
- DOI: 10.1097/SLA.0000000000005662
Actionable Factors Fostering Health Value Generation and Scalability of Prehabilitation: A Prospective Cohort Study
Abstract
Importance: Prehabilitation has potential for improving surgical outcomes as shown in previous randomized controlled trials. However, a marked efficacy-effectiveness gap is limiting its scalability. Comprehensive analyses of deployment of the intervention in real-life scenarios are required.
Objective: To assess health outcomes and cost of prehabilitation.
Design: Prospective cohort study with a control group built using propensity score-matching techniques.
Setting: Prehabilitation Unit in a tertiary-care university hospital.
Participants: Candidates for major digestive, cardiac, thoracic, gynecologic, or urologic surgeries.
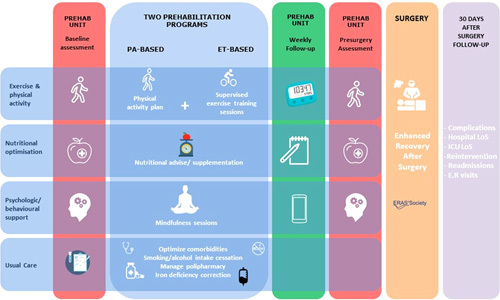
Intervention: Prehabilitation program, including supervised exercise training, promotion of physical activity, nutritional optimization, and psychological support.
Main outcomes and measures: The comprehensive complication index, hospital and intensive care unit length of stay, and hospital costs per patient until 30 days after surgery. Patients were classified by the degree of program completion and level of surgical aggression for sensitivity analysis.
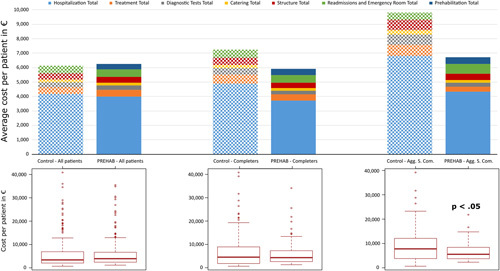
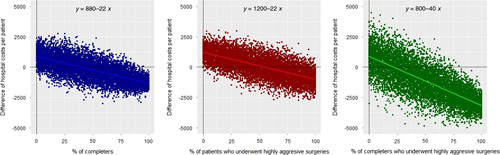
Results: The analysis of the entire study group did not show differences in study outcomes between prehabilitation and control groups (n=328 each). The per-protocol analysis, including only patients completing the program (n=112, 34%), showed a reduction in mean hospital stay [9.9 (7.2) vs 12.8 (12.4) days; P =0.035]. Completers undergoing highly aggressive surgeries (n=60) additionally showed reduction in mean intensive care unit stay [2.3 (2.7) vs 3.8 (4.2) days; P =0.021] and generated mean cost savings per patient of €3092 (32% cost reduction) ( P =0.007). Five priority areas for action to enhance service efficiencies were identified.
Conclusions and relevance: The study indicates a low rate of completion of the intervention and identifies priority areas for re-design of service delivery to enhance the effectiveness of prehabilitation.
Copyright © 2022 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Nepogodiev D, Martin J, Biccard B, et al. Global burden of postoperative death. Lancet. 2019;393:401. - PubMed
-
- Weiser TG, Regenbogen SE, Thompson KD, et al. An estimation of the global volume of surgery: a modelling strategy based on available data. Lancet. 2008;372:139–144. - PubMed
-
- Snowden CP, Prentis J, Jacques B, et al. Cardiorespiratory fitness predicts mortality and hospital length of stay after major elective surgery in older people. Ann Surg. 2013;257:999–1004. - PubMed
-
- Sepehri A, Beggs T, Hassan A, et al. The impact of frailty on outcomes after cardiac surgery: a systematic review. J Thorac Cardiovasc Surg. 2014;148:3110–3117. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
