

Non-invasive diagnosis and surveillance of bladder cancer with driver and passenger DNA methylation in a prospective cohort study
- PMID: 35968916
- PMCID: PMC9377153
- DOI: 10.1002/ctm2.1008
Non-invasive diagnosis and surveillance of bladder cancer with driver and passenger DNA methylation in a prospective cohort study
Abstract
Background: State-of-art non-invasive diagnosis processes for bladder cancer (BLCA) harbour shortcomings such as low sensitivity and specificity, unable to distinguish between high- (HG) and low-grade (LG) tumours, as well as inability to differentiate muscle-invasive bladder cancer (MIBC) and non-muscle-invasive bladder cancer (NMIBC). This study investigates a comprehensive characterization of the entire DNA methylation (DNAm) landscape of BLCA to determine the relevant biomarkers for the non-invasive diagnosis of BLCA.
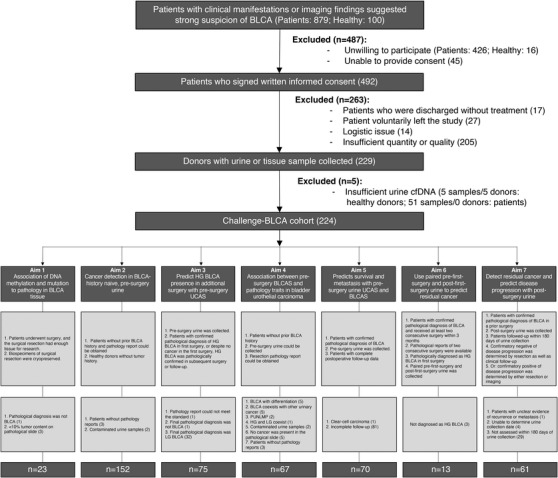
Methods: A total of 304 samples from 224 donors were enrolled in this multi-centre, prospective cohort study. BLCA-specific DNAm signature discovery was carried out with genome-wide bisulfite sequencing in 32 tumour tissues and 12 normal urine samples. A targeted sequencing assay for BLCA-specific DNAm signatures was developed to categorize tumour tissue against normal urine, or MIBC against NMIBC. Independent validation was performed with targeted sequencing of 259 urine samples in a double-blinded manner to determine the clinical diagnosis and prognosis value of DNAm-based classification models. Functions of genomic region harbouring BLCA-specific DNAm signature were validated with biological assays. Concordances of pathology to urine tumour DNA (circulating tumour DNA [ctDNA]) methylation, genomic mutations or other state-of-the-art diagnosis methods were measured.
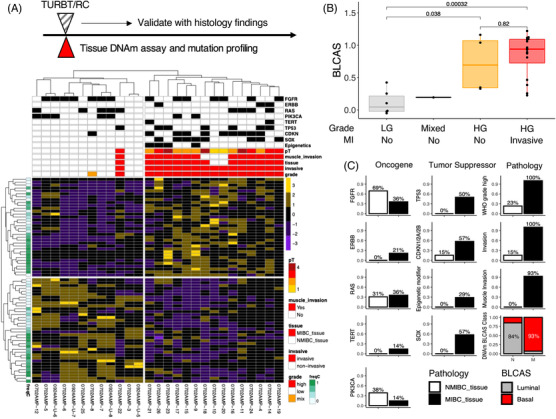
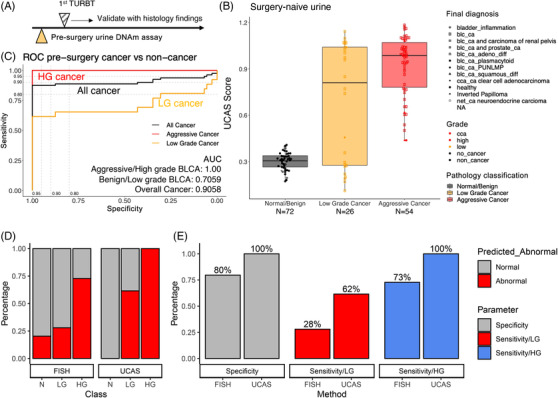
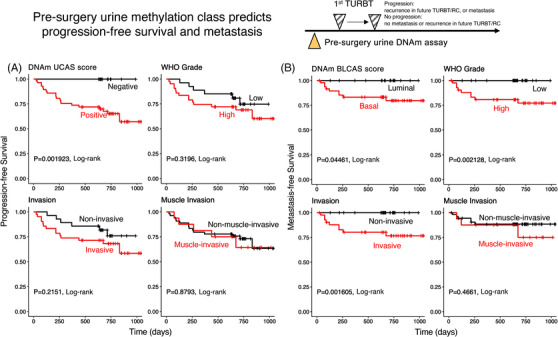
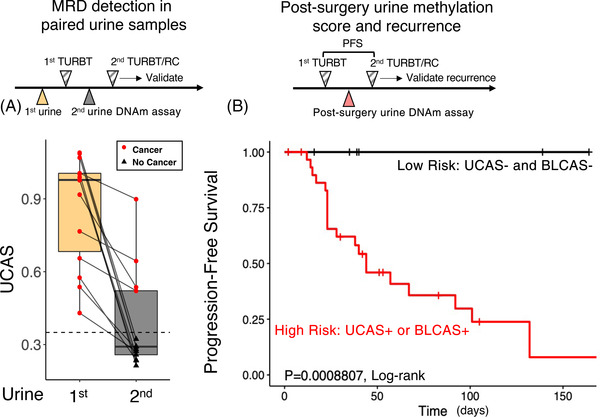
Results: Genome-wide DNAm profile could accurately classify LG tumour from HG tumour (LG NMIBC vs. HG NMIBC: p = .038; LG NMIBC vs. HG MIBC, p = .00032; HG NMIBC vs. HG MIBC: p = .82; Student's t-test). Overall, the DNAm profile distinguishes MIBC from NMIBC and normal urine. Targeted-sequencing-based DNAm signature classifiers accurately classify LG NMIBC tissues from HG MIBC and could detect tumours in urine at a limit of detection of less than .5%. In tumour tissues, DNAm accurately classifies pathology, thus outperforming genomic mutation or RNA expression profiles. In the independent validation cohort, pre-surgery urine ctDNA methylation outperforms fluorescence in situ hybridization (FISH) assay to detect HG BLCA (n = 54) with 100% sensitivity (95% CI: 82.5%-100%) and LG BLCA (n = 26) with 62% sensitivity (95% CI: 51.3%-72.7%), both at 100% specificity (non-BLCA: n = 72; 95% CI: 84.1%-100%). Pre-surgery urine ctDNA methylation signature correlates with pathology and predicts recurrence and metastasis. Post-surgery urine ctDNA methylation (n = 61) accurately predicts recurrence-free survival within 180 days, with 100% accuracy.
Conclusion: With the discovery of BLCA-specific DNAm signatures, targeted sequencing of ctDNA methylation outperforms FISH and DNA mutation to detect tumours, predict recurrence and make prognoses.
Keywords: bladder cancer; diagnosis and prognosis; methylation; non-invasive screening; prospective cohort study; urine tumour DNA.
© 2022 The Authors. Clinical and Translational Medicine published by John Wiley & Sons Australia, Ltd on behalf of Shanghai Institute of Clinical Bioinformatics.
Conflict of interest statement
All authors declare that they have no conflict of interest or financial conflicts to disclose.
Figures
Similar articles
-
Methylation of HOXA9 and ISL1 Predicts Patient Outcome in High-Grade Non-Invasive Bladder Cancer.PLoS One. 2015 Sep 2;10(9):e0137003. doi: 10.1371/journal.pone.0137003. eCollection 2015. PLoS One. 2015. PMID: 26332997 Free PMC article.
-
Mutational Analysis of 472 Urothelial Carcinoma Across Grades and Anatomic Sites.Clin Cancer Res. 2019 Apr 15;25(8):2458-2470. doi: 10.1158/1078-0432.CCR-18-3147. Epub 2018 Dec 28. Clin Cancer Res. 2019. PMID: 30593515
-
Promoter methylation of DNA damage repair (DDR) genes in human tumor entities: RBBP8/CtIP is almost exclusively methylated in bladder cancer.Clin Epigenetics. 2018 Feb 6;10:15. doi: 10.1186/s13148-018-0447-6. eCollection 2018. Clin Epigenetics. 2018. PMID: 29445424 Free PMC article.
-
Circulating Tumour DNA in Muscle-Invasive Bladder Cancer.Int J Mol Sci. 2018 Aug 29;19(9):2568. doi: 10.3390/ijms19092568. Int J Mol Sci. 2018. PMID: 30158468 Free PMC article. Review.
-
DNA methylation-based biomarkers in bladder cancer.Nat Rev Urol. 2013 Jun;10(6):327-35. doi: 10.1038/nrurol.2013.89. Epub 2013 Apr 30. Nat Rev Urol. 2013. PMID: 23628807 Review.
Cited by
-
Liquid biopsy: Comprehensive overview of circulating tumor DNA (Review).Oncol Lett. 2024 Sep 13;28(5):548. doi: 10.3892/ol.2024.14681. eCollection 2024 Nov. Oncol Lett. 2024. PMID: 39319213 Free PMC article. Review.
-
Unveiling clinical significance and tumor immune landscape of CXCL12 in bladder cancer: Insights from multiple omics analysis.Chin J Cancer Res. 2023 Dec 30;35(6):686-701. doi: 10.21147/j.issn.1000-9604.2023.06.12. Chin J Cancer Res. 2023. PMID: 38204439 Free PMC article.
-
Brain Tumor Classification by Methylation Profile.J Korean Med Sci. 2023 Nov 6;38(43):e356. doi: 10.3346/jkms.2023.38.e356. J Korean Med Sci. 2023. PMID: 37935168 Free PMC article. Review.
-
Hypermethylation Loci of ZNF671, IRF8, and OTX1 as Potential Urine-Based Predictive Biomarkers for Bladder Cancer.Diagnostics (Basel). 2024 Feb 21;14(5):468. doi: 10.3390/diagnostics14050468. Diagnostics (Basel). 2024. PMID: 38472940 Free PMC article.
-
From Detection to Cure - Emerging Roles for Urinary Tumor DNA (utDNA) in Bladder Cancer.Curr Oncol Rep. 2024 Aug;26(8):945-958. doi: 10.1007/s11912-024-01555-0. Epub 2024 Jun 5. Curr Oncol Rep. 2024. PMID: 38837106 Review.
References
-
- Babjuk M, Burger M, Comperat EM, et al. European association of urology guidelines on non‐muscle‐invasive bladder cancer (TaT1 and carcinoma in situ) – 2019 update. Eur Urol. 2019;76:639‐657. - PubMed
-
- Witjes JA, Bruins HM, Cathomas R, et al. European association of urology guidelines on muscle‐invasive and metastatic bladder cancer: summary of the 2020 guidelines. Eur Urol. 2021;79:82‐104. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical