

A case of esophageal atresia with the bronchial-like lower esophagus which originates from the left lower lobe bronchus
- PMID: 35969287
- PMCID: PMC9378802
- DOI: 10.1186/s40792-022-01513-7
A case of esophageal atresia with the bronchial-like lower esophagus which originates from the left lower lobe bronchus
Abstract
Background: Esophageal atresia with or without a trachea-esophageal fistula occurs due to the failure of separation or incomplete development of the foregut. Therefore, esophageal atresia is often associated with various forms of tracheobronchial anomalies. We report an extremely rare case of esophageal atresia.
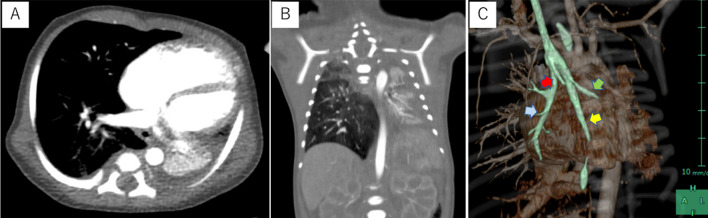
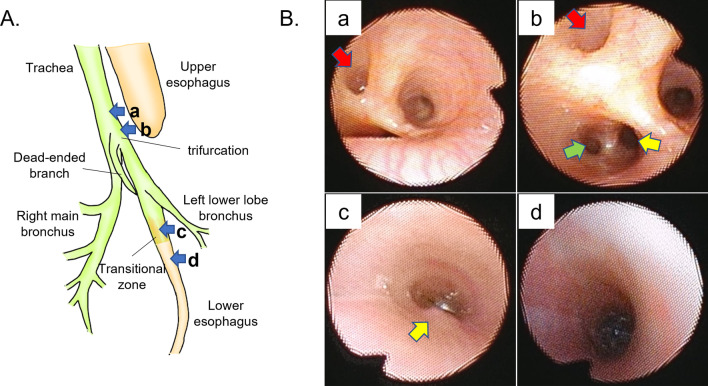
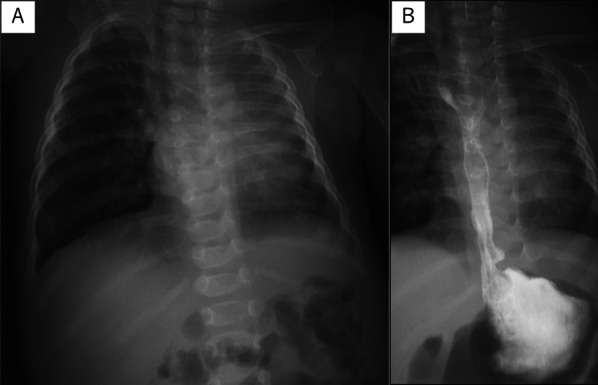
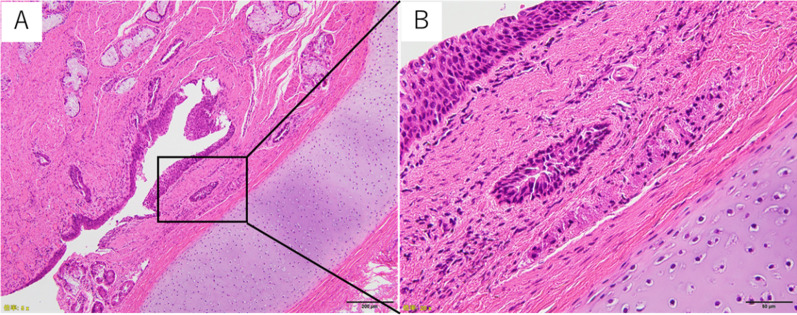
Case presentation: A female infant was born at 37 weeks of gestation and weighed 2596 g. A diagnosis of esophageal atresia and total anomalous pulmonary vein return type III were confirmed. The infant had respiratory distress that required tracheal intubation and ventilatory support soon after birth. Temporary banding of the gastroesophageal junction and gastrostomy were performed on the second day of life. However, her respiratory condition deteriorated due to atelectasis of the left lung and compensatory hyperinflation of the right lung. Preoperative examinations showed the unilobe and atelectatic left lung. The trachea was trifurcated in three directions, and the branch that was expected to be the left main bronchus was blind-ended. The dorsal branch was cartilaginous and bifurcated into the left lower lobe bronchus and lower esophagus approximately 1 cm distal from the tracheal trifurcation. The cartilaginous tissue continued to the lower esophagus. The diagnosis of esophageal atresia with the lower esophagus which originated from the left lower lobe bronchus was made. Esophageal atresia repair was performed when the patient was 4 months of age. The esophagus was dissected distally to the bifurcation of the left lower lobe bronchus via right thoracotomy. The lower esophagus was bronchial-like in appearance, transitioning to the normal esophageal wall approximately 7 mm distal to the transected edge. The cartilage tissue was completely resected during surgery, and a primary end-to-end anastomosis of the esophagus was successfully performed. Histopathological findings revealed that the extracted specimen was surrounded by tracheal cartilage and that the inner surface was covered by stratified squamous epithelium that originated from the esophagus.
Conclusions: In cases of esophageal atresia with an atypical clinical presentation, there may be unique structural abnormalities of the foregut. We emphasize the importance of a preoperative surgical planning since an inadequate operation can lead to fatal complications.
Keywords: Broncho-esophageal fistula; Communicating bronchopulmonary foregut malformation; Esophageal atresia.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that there are no competing interests regarding the publication of this paper.
Figures

References
LinkOut - more resources
Full Text Sources
