

Association Between Standardized Mortality Ratio and Utilization of Care in US Veterans With Drug-Resistant Epilepsy Compared With All US Veterans and the US General Population
- PMID: 35969384
- PMCID: PMC9379823
- DOI: 10.1001/jamaneurol.2022.2290
Association Between Standardized Mortality Ratio and Utilization of Care in US Veterans With Drug-Resistant Epilepsy Compared With All US Veterans and the US General Population
Abstract
Importance: Drug-resistant epilepsy (DRE) is thought to be associated with increased mortality, but larger population-based studies are lacking. Additionally, the benefit of effective management in DRE lacks evidence.
Objective: To examine the association of utilization of care with mortality in US veterans with DRE.
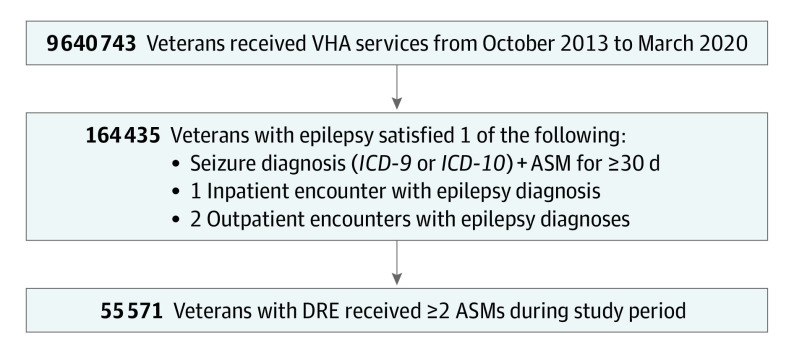
Design, setting, and participants: Observational cohort study conducted between October 1, 2013, and March 31, 2020. Mortality statistics in US veterans with DRE were compared to the US general population and all veterans within the Veterans Health Administration. Epilepsy was defined as use of 1 or more antiseizure medications (ASMs) for 30 days or longer with a seizure diagnosis or 1 inpatient or 2 outpatient encounters with an epilepsy diagnosis. DRE was defined as the use of 2 or more ASMs. Among 9.6 million US veterans, 164 435 (1.7%) had epilepsy, of whom 55 571 (33.8%) had DRE. Epilepsy and DRE were administratively identified based on criteria noted in design. Identified participants were included for analysis.
Exposures: Veterans with DRE.
Main outcomes and measures: Standardized mortality ratio (SMR).
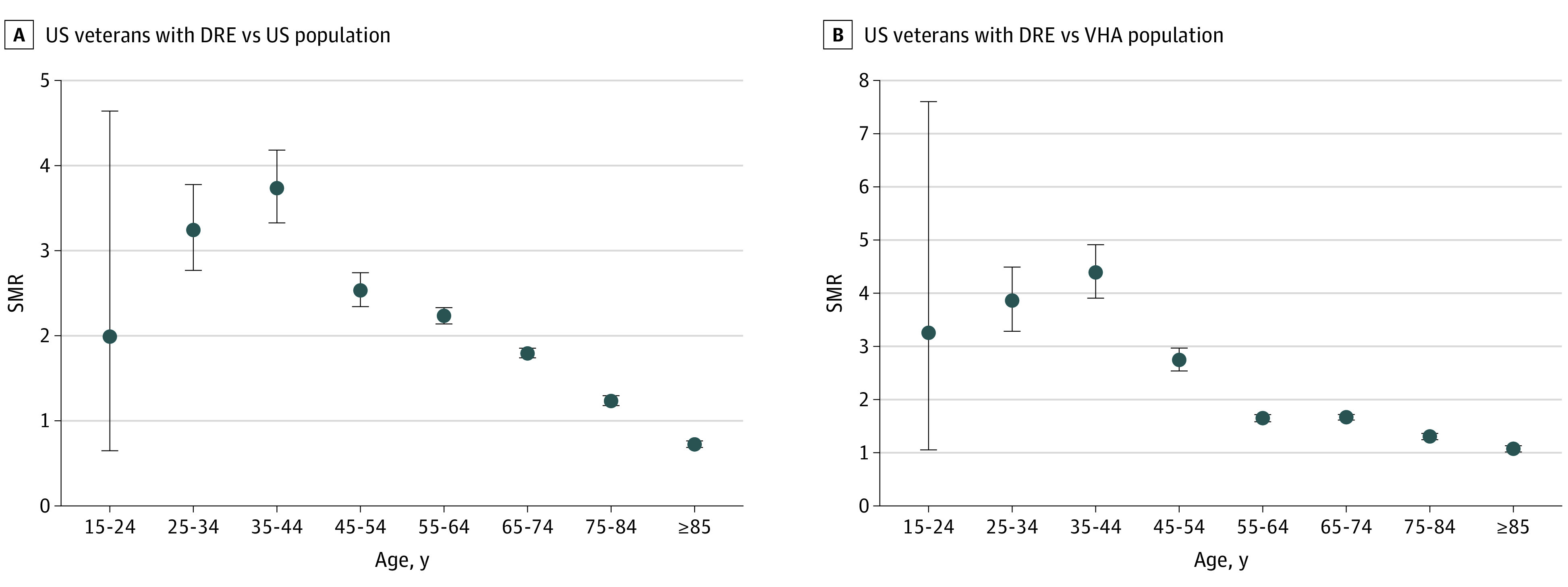
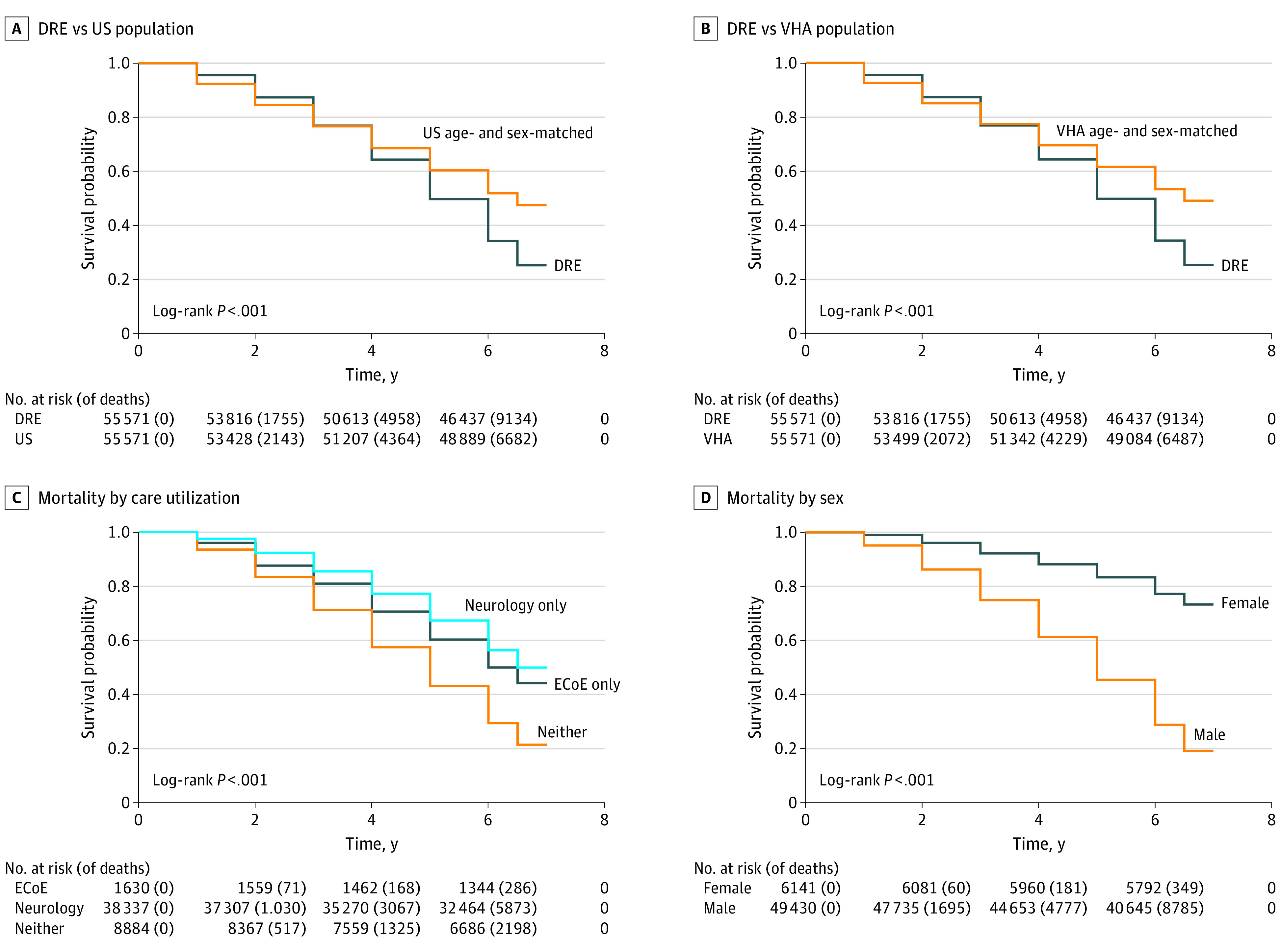
Results: Among US veterans with DRE, the mean (SD) age was 58.3 (15.4) years, and 49 430 individuals (88.9%) were male. Of ethnicity data gathered, 3170 individuals (5.7%) were Hispanic or Latino, 50 599 (91.1%) were not Hispanic or Latino, 842 (1.5%) declined to answer, and 960 (1.7%) were recorded as unknown. Of race data gathered, 516 individuals (0.9%) were American Indian or Alaskan Native, 270 (0.5%) were Asian, 11 316 (20.4%) were Black or African American, 587 (1.1%) were of multiple races, 453 (0.8%) were Native Hawaiian or Pacific Islander, 39 543 (71.2%) were White, 1697 (3.1%) declined to answer, and 1189 (2.1%) were recorded as unknown. SMR was 1.50 (95% CI, 1.47-1.53) compared with the US general population and 1.56 (95% CI, 1.53-1.59) compared with all veterans. Utilization rates were 81.1% (n = 45 057) for neurology clinic evaluation, 66.4% (n = 36 905) for magnetic resonance imaging (MRI), and 49.6% (n = 27 546) for electroencephalography (EEG) testing. Only 8350 individuals (15.0%) had comprehensive epilepsy evaluations and 3357 (6.0%) had epilepsy monitoring. Multivariable analysis revealed an association between lower mortality and neurology clinic evaluation, EEG, MRI, epilepsy monitoring, and the use of more than 2 ASMs after adjusting for age and comorbidities.
Conclusions and relevance: Mortality rates were significantly higher in US veterans with DRE compared to the general population. Better utilization of comprehensive epilepsy care, diagnostic services, and medications were each associated with reduced mortality. These findings indicate that appropriate management of DRE is critical in this population.
Conflict of interest statement
Figures
Similar articles
-
Survival Outcomes by Race and Ethnicity in Veterans With Nonmetastatic Castration-Resistant Prostate Cancer.JAMA Netw Open. 2023 Oct 2;6(10):e2337272. doi: 10.1001/jamanetworkopen.2023.37272. JAMA Netw Open. 2023. PMID: 37819658 Free PMC article.
-
Association of Race and Ethnicity With Prescription of SGLT2 Inhibitors and GLP1 Receptor Agonists Among Patients With Type 2 Diabetes in the Veterans Health Administration System.JAMA. 2022 Sep 6;328(9):861-871. doi: 10.1001/jama.2022.13885. JAMA. 2022. PMID: 36066519 Free PMC article.
-
Optimizing drug-resistant epilepsy identification in the Veterans Health Administration.Epilepsy Res. 2025 Aug;214:107568. doi: 10.1016/j.eplepsyres.2025.107568. Epub 2025 Apr 22. Epilepsy Res. 2025. PMID: 40300417
-
Value contribution of cenobamate for the treatment of Focal-Onset Seizures (FOS) in patients with drug-resistant epilepsy (DRE) in Spain through reflective Multi-Criteria Decision Analysis (MCDA).Epilepsy Behav. 2023 Aug;145:109350. doi: 10.1016/j.yebeh.2023.109350. Epub 2023 Jul 20. Epilepsy Behav. 2023. PMID: 37480633
-
Identifying key unmet needs and value drivers in the treatment of focal-onset seizures (FOS) in patients with drug-resistant epilepsy (DRE) in Spain through Multi-Criteria Decision Analysis (MCDA).Epilepsy Behav. 2021 Sep;122:108222. doi: 10.1016/j.yebeh.2021.108222. Epub 2021 Aug 6. Epilepsy Behav. 2021. PMID: 34371462
