

Association of Methamphetamine and Opioid Use With Nonfatal Overdose in Rural Communities
- PMID: 35969400
- PMCID: PMC9379740
- DOI: 10.1001/jamanetworkopen.2022.26544
Association of Methamphetamine and Opioid Use With Nonfatal Overdose in Rural Communities
Abstract
Importance: Overdoses continue to increase in the US, but the contribution of methamphetamine use is understudied in rural communities.
Objective: To estimate the prevalence of methamphetamine use and its correlates among people who use drugs (PWUD) in rural US communities and to determine whether methamphetamine use is associated with increased nonfatal overdoses.
Design, setting, and participants: From January 2018 through March 2020, the National Rural Opioid Initiative conducted cross-sectional surveys of PWUD in rural communities in 10 states (Illinois, Kentucky, New Hampshire, Massachusetts, North Carolina, Ohio, Oregon, Vermont, West Virginia, and Wisconsin). Participants included rural PWUD who reported any past-30-day injection drug use or noninjection opioid use to get high. A modified chain-referral sampling strategy identified seeds who referred others using drugs. Data analysis was performed from May 2021 to January 2022.
Exposures: Use of methamphetamine alone, opioids alone, or both.
Main outcomes and measures: Unweighted and weighted prevalence of methamphetamine use, any past-180-day nonfatal overdose, and number of lifetime nonfatal overdoses.
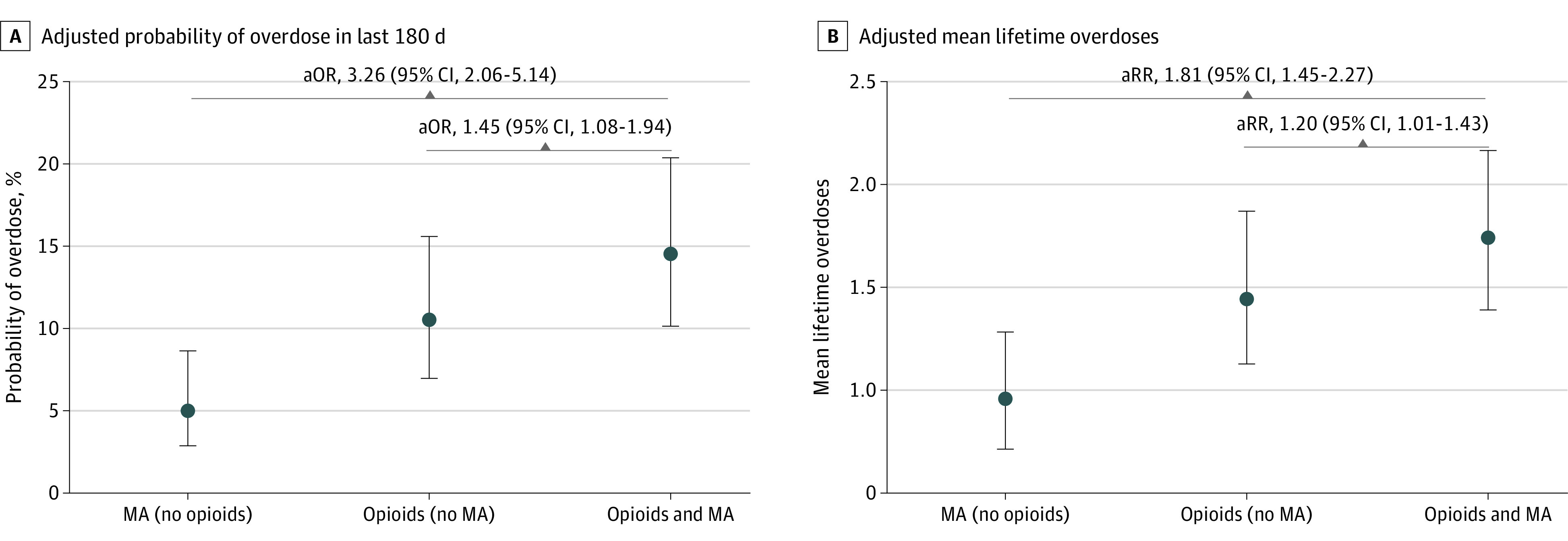
Results: Among the 3048 participants, 1737 (57%) were male, 2576 (85%) were White, and 225 (7.4%) were American Indian; the mean (SD) age was 36 (10) years. Most participants (1878 of 2970 participants with any opioid or methamphetamine use [63%]) reported co-use of methamphetamine and opioids, followed by opioids alone (702 participants [24%]), and methamphetamine alone (390 participants [13%]). The estimated unweighted prevalence of methamphetamine use was 80% (95% CI, 64%-90%), and the estimated weighted prevalence was 79% (95% CI, 57%-91%). Nonfatal overdose was greatest in people using both methamphetamine and opioids (395 of 2854 participants with nonmissing overdose data [22%]) vs opioids alone (99 participants [14%]) or methamphetamine alone (23 participants [6%]). Co-use of methamphetamine and opioids was associated with greater nonfatal overdose compared with opioid use alone (adjusted odds ratio, 1.45; 95% CI, 1.08-1.94; P = .01) and methamphetamine use alone (adjusted odds ratio, 3.26; 95% CI, 2.06-5.14; P < .001). Those with co-use had a mean (SD) of 2.4 (4.2) (median [IQR], 1 [0-3]) lifetime overdoses compared with 1.7 (3.5) (median [IQR], 0 [0-2]) among those using opioids alone (adjusted rate ratio, 1.20; 95% CI, 1.01-1.43; P = .04), and 1.1 (2.9) (median [IQR], 0 [0-1]) among those using methamphetamine alone (adjusted rate ratio, 1.81; 95% CI, 1.45-2.27; P < .001). Participants with co-use most often reported having tried and failed to access substance use treatment: 827 participants (44%) for both, 117 participants (30%) for methamphetamine alone, and 252 participants (36%) for opioids alone (χ22 = 33.8; P < .001). Only 66 participants (17%) using methamphetamine alone had naloxone.
Conclusions and relevance: These findings suggest that harm reduction and substance use disorder treatment interventions must address both methamphetamine and opioids to decrease overdose in rural communities.
Conflict of interest statement
Figures
References
-
- Ahmad FB, Rossen LM, Sutton P. Provisional drug overdose death counts. National Center for Health Statistics. Updated February 9, 2022. Accessed January 10, 2022. https://www.cdc.gov/nchs/nvss/vsrr/drug-overdose-data.htm
-
- Gladden RM, O’Donnell J, Mattson CL, Seth P. Changes in opioid-involved overdose deaths by opioid type and presence of benzodiazepines, cocaine, and methamphetamine: 25 states, July-December 2017 to January-June 2018. MMWR Morb Mortal Wkly Rep. 2019;68(34):737-744. doi: 10.15585/mmwr.mm6834a2 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- UG3 DA044831/DA/NIDA NIH HHS/United States
- UG3 DA044825/DA/NIDA NIH HHS/United States
- UH3 DA044822/DA/NIDA NIH HHS/United States
- K23 DA053390/DA/NIDA NIH HHS/United States
- UG3 DA044798/DA/NIDA NIH HHS/United States
- UH3 DA044826/DA/NIDA NIH HHS/United States
- U24 DA048538/DA/NIDA NIH HHS/United States
- UH3 DA044823/DA/NIDA NIH HHS/United States
- UH3 DA044830/DA/NIDA NIH HHS/United States
- K01 DA055130/DA/NIDA NIH HHS/United States
- UG3 DA044822/DA/NIDA NIH HHS/United States
- F31 DA054752/DA/NIDA NIH HHS/United States
- UH3 DA044798/DA/NIDA NIH HHS/United States
- UH3 DA044829/DA/NIDA NIH HHS/United States
- UG3 DA044826/DA/NIDA NIH HHS/United States
- UG3 DA044823/DA/NIDA NIH HHS/United States
- UH3 DA044831/DA/NIDA NIH HHS/United States
- UG3 DA044830/DA/NIDA NIH HHS/United States
- UG3 DA044829/DA/NIDA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
