

Virologic Efficacy of Casirivimab and Imdevimab COVID-19 Antibody Combination in Outpatients With SARS-CoV-2 Infection: A Phase 2 Dose-Ranging Randomized Clinical Trial
- PMID: 35969402
- PMCID: PMC9379747
- DOI: 10.1001/jamanetworkopen.2022.25411
Virologic Efficacy of Casirivimab and Imdevimab COVID-19 Antibody Combination in Outpatients With SARS-CoV-2 Infection: A Phase 2 Dose-Ranging Randomized Clinical Trial
Abstract
Importance: The monoclonal antibody combination of casirivimab and imdevimab reduced viral load, hospitalization, or death when administered as a 1200-mg or greater intravenous (IV) dose in a phase 3 COVID-19 outpatient study. Subcutaneous (SC) and/or lower IV doses should increase accessibility and/or drug supplies for patients.
Objective: To assess the virologic efficacy of casirivimab and imdevimab across different IV and SC doses compared with placebo.
Design, setting, and participants: This phase 2, randomized, double-blind, placebo-controlled, parallel-group, dose-ranging study included outpatients with SARS-CoV-2 infection at 47 sites across the United States. Participants could be symptomatic or asymptomatic; symptomatic patients with risk factors for severe COVID-19 were excluded. Data were collected from December 15, 2020, to March 4, 2021.
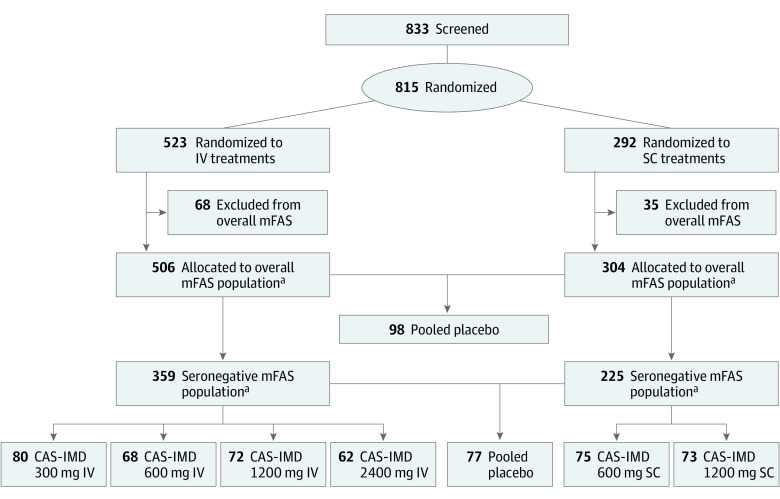
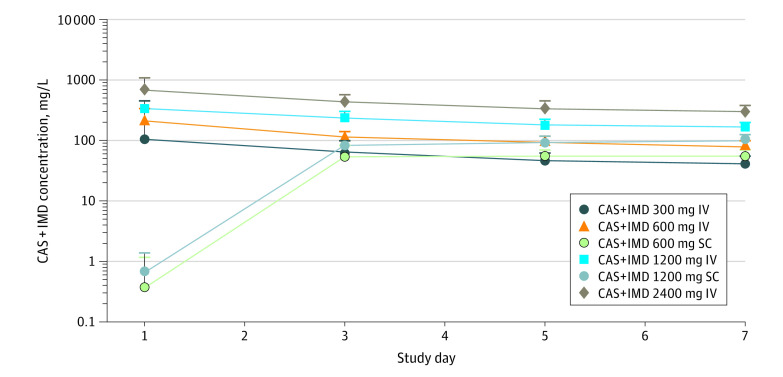
Interventions: Patients were randomized to a single IV dose (523 patients) of casirivimab and imdevimab at 300, 600, 1200, or 2400 mg or placebo; or a single SC dose (292 patients) of casirivimab and imdevimab at 600 or 1200 mg or placebo.
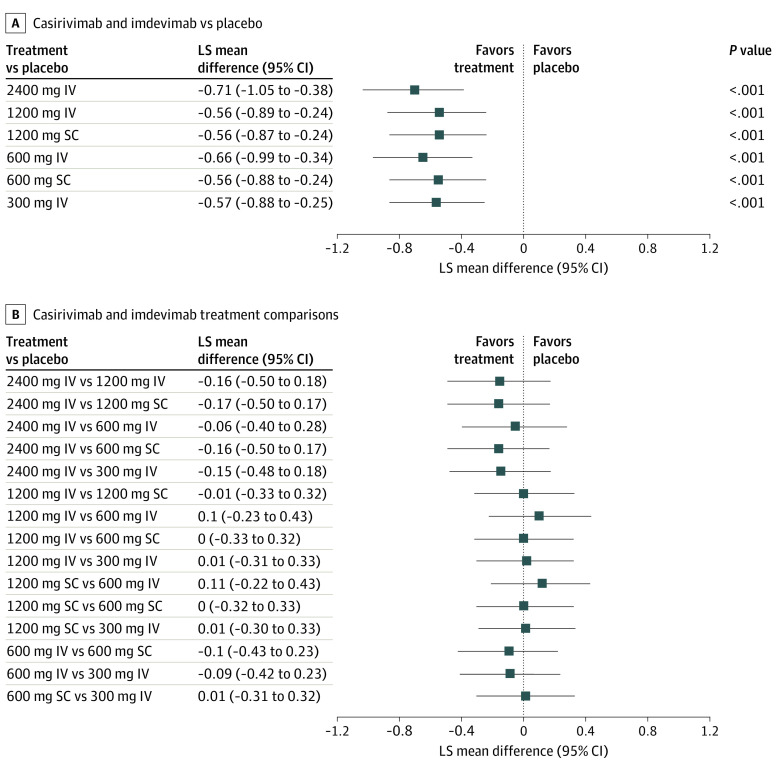
Main outcomes and measures: The primary end point was the time-weighted average daily change from baseline (TWACB) in viral load from day 1 (baseline) through day 7 in patients seronegative for SARS-CoV-2 at baseline.
Results: Among 815 randomized participants, 507 (282 randomized to IV treatment, 148 randomized to SC treatment, and 77 randomized to placebo) were seronegative at baseline and included in the primary efficacy analysis. Participants randomized to IV had a mean (SD) age of 34.6 (9.6) years (160 [44.6%] men; 14 [3.9%] Black; 121 [33.7%] Hispanic or Latino; 309 [86.1%] White); those randomized to SC had a mean age of 34.1 (10.0) years (102 [45.3%] men; 75 [34.7%] Hispanic or Latino; 6 [2.7%] Black; 190 [84.4%] White). All casirivimab and imdevimab treatments showed significant virologic reduction through day 7. Least-squares mean differences in TWACB viral load for casirivimab and imdevimab vs placebo ranged from -0.56 (95% CI; -0.89 to -0.24) log10 copies/mL for the 1200-mg IV dose to -0.71 (95% CI, -1.05 to -0.38) log10 copies/mL for the 2400-mg IV dose. There were no adverse safety signals or dose-related safety findings, grade 2 or greater infusion-related or hypersensitivity reactions, grade 3 or greater injection-site reactions, or fatalities. Two serious adverse events not related to COVID-19 or the study drug were reported.
Conclusions and relevance: In this randomized clinical trial including outpatients with asymptomatic and low-risk symptomatic SARS-CoV-2, all IV and SC doses of casirivimab and imdevimab comparably reduced viral load.
Trial registration: ClinicalTrials.gov Identifier: NCT04666441.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
