

Neoadjuvant Nivolumab Plus Ipilimumab and Adjuvant Nivolumab in Localized Deficient Mismatch Repair/Microsatellite Instability-High Gastric or Esophagogastric Junction Adenocarcinoma: The GERCOR NEONIPIGA Phase II Study
- PMID: 35969830
- PMCID: PMC9839243
- DOI: 10.1200/JCO.22.00686
Neoadjuvant Nivolumab Plus Ipilimumab and Adjuvant Nivolumab in Localized Deficient Mismatch Repair/Microsatellite Instability-High Gastric or Esophagogastric Junction Adenocarcinoma: The GERCOR NEONIPIGA Phase II Study
Abstract
Purpose: In patients with resectable gastric/gastroesophageal junction (GEJ) adenocarcinoma, surgery plus perioperative platinum-based chemotherapy is the standard of care. Perioperative chemotherapy remains debatable for gastric/GEJ adenocarcinoma with deficient mismatch repair (dMMR)/microsatellite instability-high (MSI-H).
Patients and methods: NEONIPIGA (ClinicalTrials.gov identifier: NCT04006262) phase II study evaluated neoadjuvant nivolumab 240 mg once every two weeks ×6 and ipilimumab 1 mg/kg once every six weeks ×2, followed by surgery and adjuvant nivolumab 480 mg once every four weeks (nine injections) in patients with locally advanced resectable dMMR/MSI-H, clinical (c) tumor (T)2-T4 node (N)x metastasis (M)0 gastric/GEJ adenocarcinoma. The primary end point was a pathological complete response (pCR) rate.
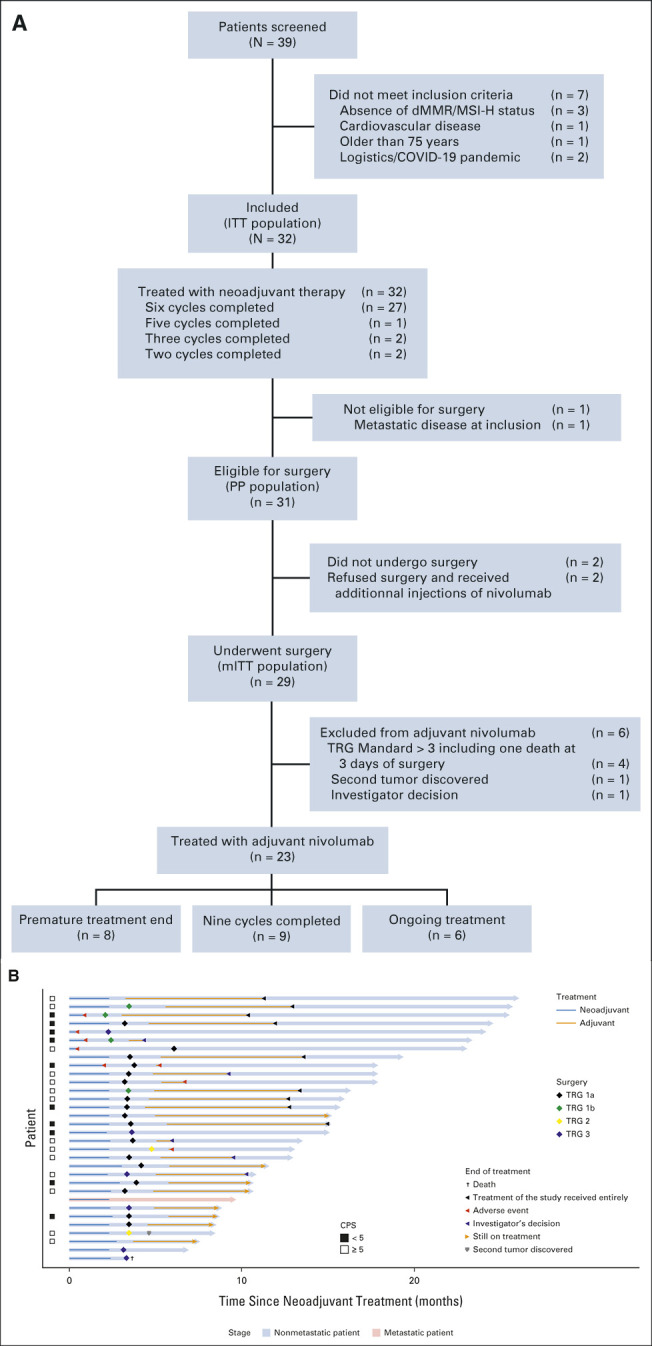
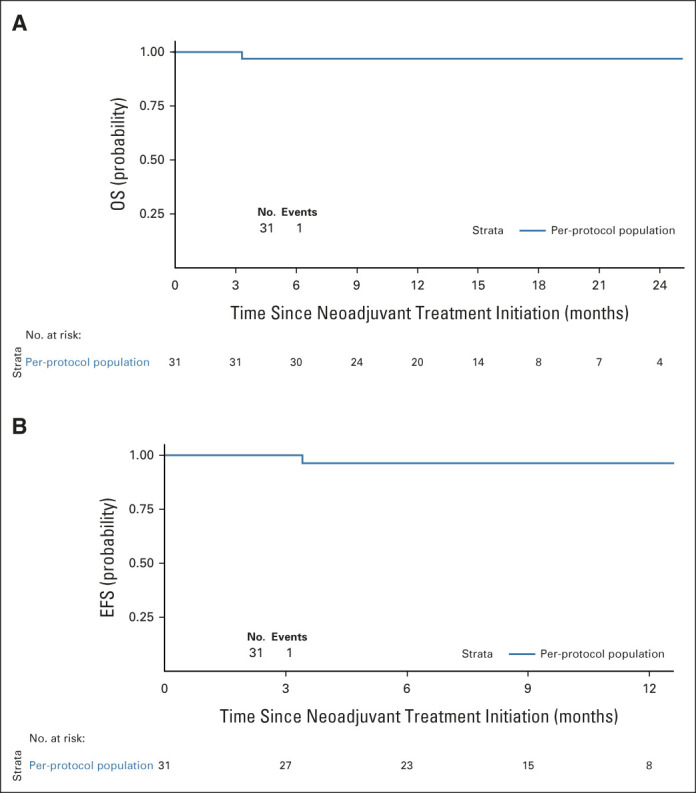
Results: Between October 2019 and June 2021, 32 patients with dMMR/MSI-H gastric/GEJ adenocarcinoma were enrolled. The median age was 65.5 years (range, 40-80). Clinical stages were cT2-T3N0 (n = 9), cT2-T3N1 (n = 22), and cT3N1M1 (n = 1, wrongly included). With a median follow-up of 14.9 months (95% CI, 10.6 to 17.6), 32 patients received neoadjuvant immunotherapy (27 patients completed all cycles). Neoadjuvant therapy-related grade 3/4 adverse events occurred in six patients (19%). Twenty-nine patients underwent surgery; three did not have surgery and had complete endoscopic response with tumor-free biopsies and a normal computed tomography scan (two refused surgery and one had metastasis at inclusion). The rate of surgical morbidity (Clavien-Dindo classification) was 55% (one postoperative death occurred). All 29 patients had an R0 resection, and 17 (58.6%; 90% CI, 41.8 to 74.1) had pCR (pathological T0N0). Becker tumor regression grades 1a, 1b, 2, and 3 were observed in 17 patients, three (including two pathological T0N1), two, and seven patients, respectively. Of the 29 patients with surgery, 23 received adjuvant nivolumab. At database lock, no patient had relapse and one died without relapse.
Conclusion: Nivolumab and ipilimumab-based neoadjuvant therapy is feasible and associated with no unexpected toxicity and a high pCR rate in patients with dMMR/MSI-H resectable gastric/GEJ adenocarcinoma.
Conflict of interest statement
No other potential conflicts of interest were reported.
Figures
References
-
- Bray F, Ferlay J, Soerjomataram I, et al. : Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 68:394-424, 2018 - PubMed
-
- Smyth EC, Verheij M, Allum W, et al. : Gastric cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol 27:v38-v49, 2016 - PubMed
-
- Cunningham D, Allum WH, Stenning SP, et al. : Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med 355:11-20, 2006 - PubMed
-
- Al-Batran S-E, Homann N, Pauligk C, et al. : Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): A randomised, phase 2/3 trial. Lancet 393:1948, 19572019 - PubMed
-
- Choi YY, Bae JM, An JY, et al. : Is microsatellite instability a prognostic marker in gastric cancer?: A systematic review with meta-analysis: MSI and gastric cancer. J Surg Oncol 110:129-135, 2014 - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
