

Umbilical cord milking in nonvigorous infants: a cluster-randomized crossover trial
- PMID: 35970202
- PMCID: PMC9877105
- DOI: 10.1016/j.ajog.2022.08.015
Umbilical cord milking in nonvigorous infants: a cluster-randomized crossover trial
Abstract
Background: Delayed cord clamping and umbilical cord milking provide placental transfusion to vigorous newborns. Delayed cord clamping in nonvigorous newborns may not be provided owing to a perceived need for immediate resuscitation. Umbilical cord milking is an alternative, as it can be performed more quickly than delayed cord clamping and may confer similar benefits.
Objective: We hypothesized that umbilical cord milking would reduce admission to the neonatal intensive care unit compared with early cord clamping in nonvigorous newborns born between 35 and 42 weeks' gestation.
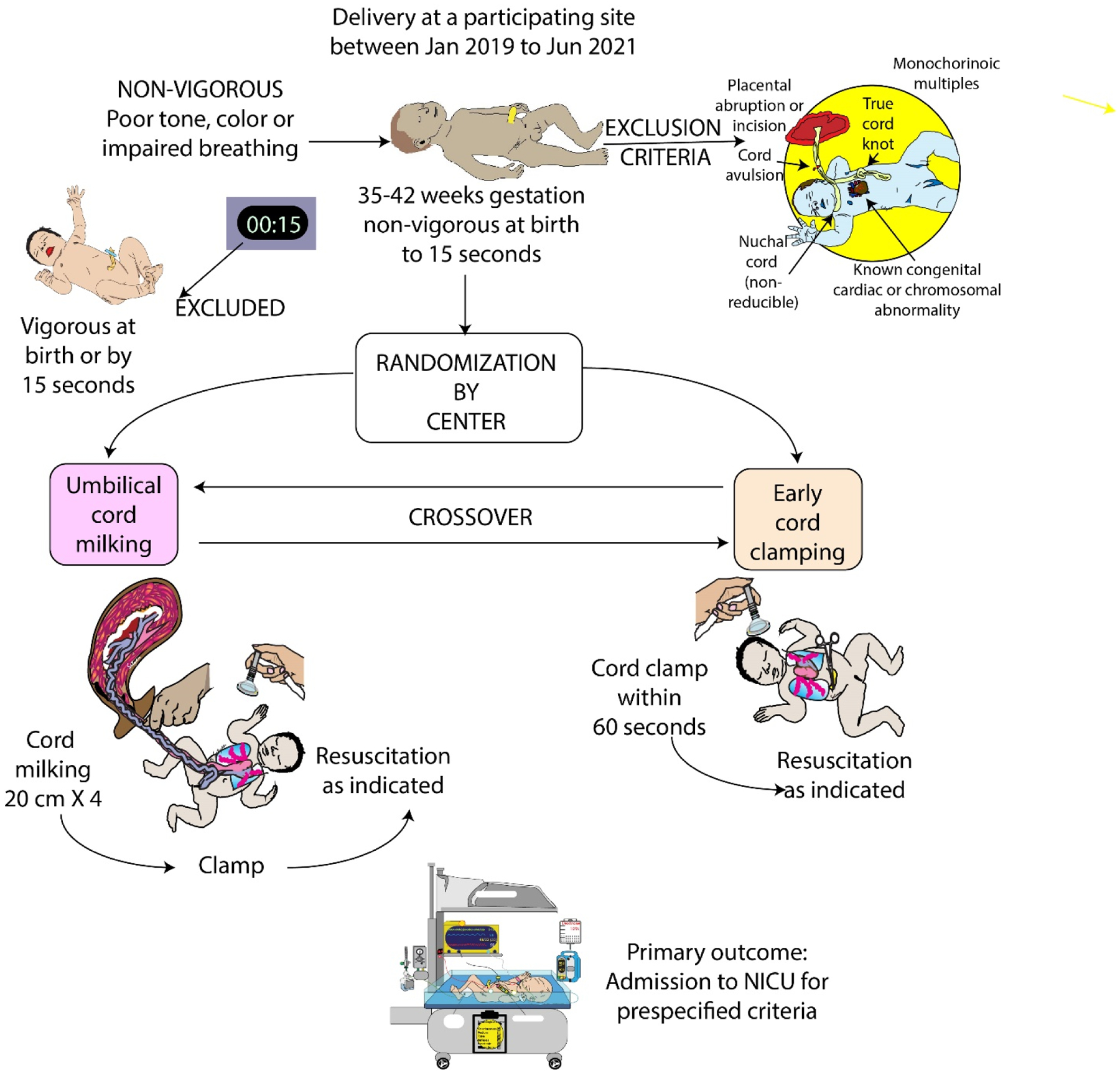
Study design: This was a pragmatic cluster-randomized crossover trial of infants born at 35 to 42 weeks' gestation in 10 medical centers in 3 countries between January 2019 and May 2021. The centers were randomized to umbilical cord milking or early cord clamping for approximately 1 year and then crossed over for an additional year or until the required number of consented subjects was reached. Waiver of consent as obtained in all centers to implement the intervention. Infants were eligible if nonvigorous at birth (poor tone, pale color, or lack of breathing in the first 15 seconds after birth) and were assigned to umbilical cord milking or early cord clamping according to their birth hospital randomization assignment. The baseline characteristics and outcomes were collected following deferred informed consent. The primary outcome was admission to the neonatal intensive care unit for predefined criteria. The main safety outcome was hypoxic-ischemic encephalopathy. Data were analyzed by the intention-to-treat concept.
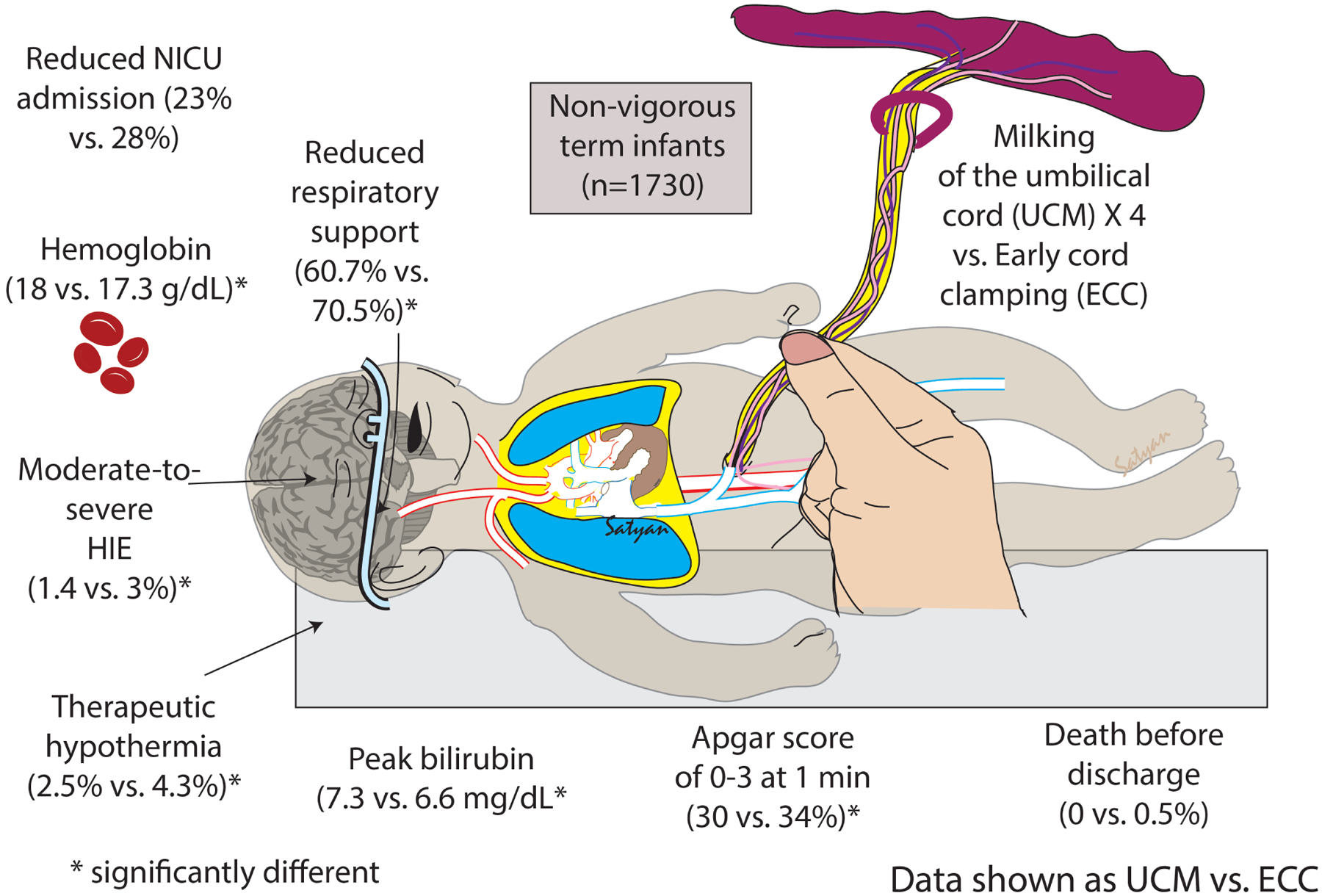
Results: Among 16,234 screened newborns, 1780 were eligible (905 umbilical cord milking, 875 early cord clamping), and 1730 had primary outcome data for analysis (97% of eligible; 872 umbilical cord milking, 858 early cord clamping) either via informed consent (606 umbilical cord milking, 601 early cord clamping) or waiver of informed consent (266 umbilical cord milking, 257 early cord clamping). The difference in the frequency of neonatal intensive care unit admission using predefined criteria between the umbilical cord milking (23%) and early cord clamping (28%) groups did not reach statistical significance (modeled odds ratio, 0.69; 95% confidence interval, 0.41-1.14). Umbilical cord milking was associated with predefined secondary outcomes, including higher hemoglobin (modeled mean difference between umbilical cord milking and early cord clamping groups 0.68 g/dL, 95% confidence interval, 0.31-1.05), lower odds of abnormal 1-minute Apgar scores (Apgar ≤3, 30% vs 34%, crude odds ratio, 0.72; 95% confidence interval, 0.56-0.92); cardiorespiratory support at delivery (61% vs 71%, modeled odds ratio, 0.57; 95% confidence interval, 0.33-0.99), and therapeutic hypothermia (3% vs 4%, crude odds ratio, 0.57; 95% confidence interval, 0.33-0.99). Moderate-to-severe hypoxic-ischemic encephalopathy was significantly less common with umbilical cord milking (1% vs 3%, crude odds ratio, 0.48; 95% confidence interval, 0.24-0.96). No significant differences were observed for normal saline bolus, phototherapy, abnormal 5-minute Apgar scores (Apgar ≤6, 15.7% vs 18.8%, crude odds ratio, 0.81; 95% confidence interval, 0.62-1.06), or a serious adverse event composite of death before discharge.
Conclusion: Among nonvigorous infants born at 35 to 42 weeks' gestation, umbilical cord milking did not reduce neonatal intensive care unit admission for predefined criteria. However, infants in the umbilical cord milking arm had higher hemoglobin, received less delivery room cardiorespiratory support, had a lower incidence of moderate-to-severe hypoxic-ischemic encephalopathy, and received less therapeutic hypothermia. These data may provide the first randomized controlled trial evidence that umbilical cord milking in nonvigorous infants is feasible, safe and, superior to early cord clamping.
Keywords: cord clamping; cord milking; newborn; nonvigorous; resuscitation.
Copyright © 2022 Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors report no conflict of interest.
Figures
Comment in
-
EBNEO commentary on "umbilical cord milking in nonvigorous infants: A cluster-randomised crossover trial".Acta Paediatr. 2023 Feb;112(2):324-325. doi: 10.1111/apa.16611. Epub 2022 Dec 10. Acta Paediatr. 2023. PMID: 36495103 No abstract available.
-
Cord milking in non-vigorous infants: promising, but further information is needed.Evid Based Nurs. 2023 Apr;26(2):77. doi: 10.1136/ebnurs-2022-103630. Epub 2022 Dec 13. Evid Based Nurs. 2023. PMID: 36600498 No abstract available.
References
-
- Wall SN, Lee ACC, Niermeyer S, English M, Keenan WJ, Carlo W, Bhutta ZA, Bang A, Narayanan I, Ariawan I, Lawn JE. Neonatal resuscitation in low-resource settings: What, who, and how to overcome challenges to scale up? International journal of gynaecology and obstetrics: the official organ of the International Federation of Gynaecology and Obstetrics. 2009;107(Suppl 1):S47–S64. doi: 10.1016/j.ijgo.2009.07.013. - DOI - PMC - PubMed
