

Preadmission Oral Anticoagulation for Atrial Fibrillation/Flutter and Death or Thrombotic Events During COVID-19 Admission
- PMID: 35970632
- PMCID: PMC9374502
- DOI: 10.1016/j.amjcard.2022.07.006
Preadmission Oral Anticoagulation for Atrial Fibrillation/Flutter and Death or Thrombotic Events During COVID-19 Admission
Abstract
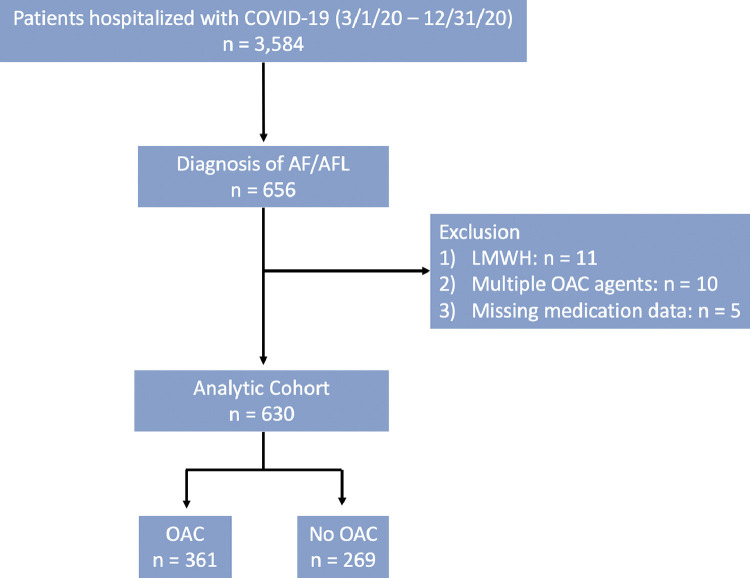
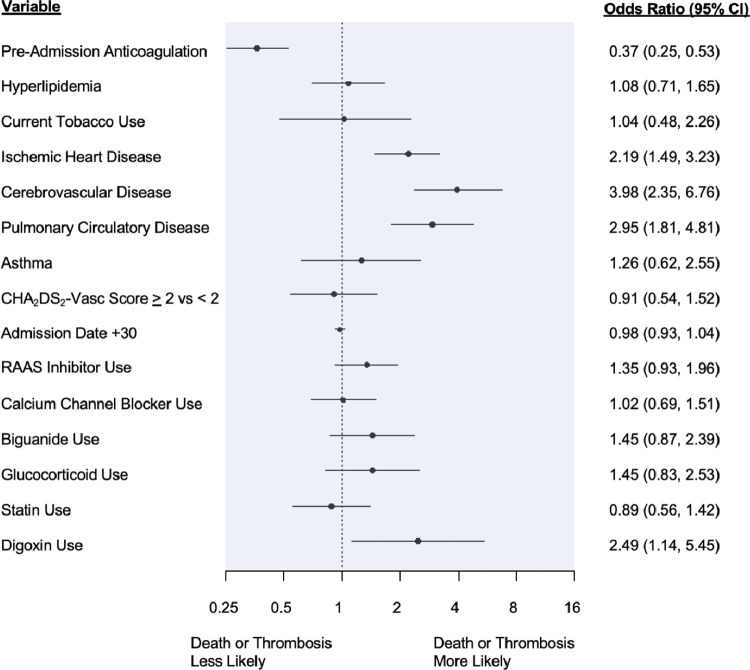
Atrial fibrillation/flutter (AF) and COVID-19 are associated with an elevated risk of arterial and venous thrombosis. Whether preadmission oral anticoagulation (OAC) for AF reduces the incidence of in-hospital death or thrombotic events among patients with COVID-19 is unknown. We identified 630 patients with pre-existing AF and a hospitalization diagnosis of COVID-19 and stratified them according to preadmission OAC use. Multivariable logistic regression was employed to relate preadmission OAC to composite in-hospital mortality or thrombotic events. Unadjusted composite in-hospital mortality or thrombotic complications occurred less often in those on than not on preadmission OAC (27.1% vs 46.8%, p <0.001). After adjustment, the incidence of composite in-hospital all-cause mortality or thrombotic complications remained lower with preadmission OAC (odds ratio 0.37, confidence interval 0.25 to 0.53, p <0.0001). Secondary outcomes including all-cause mortality (16.3% vs 24.9%, p = 0.007), intensive care unit admission (14.7% vs 29.0%, p <0.001), intubation (6.4% vs 18.6%, p <0.001), and noninvasive ventilation (18.6% vs 27.5%, p = 0.007) occurred less frequently, and length of stay was shorter (6 vs 7 days, p <0.001) in patients on than those not on preadmission OAC. A higher CHA2DS2-VASc score was associated with an increased risk of thrombotic events. In conclusion, among patients with baseline AF who were hospitalized with COVID-19, those on preadmission OAC had lower rates of death, arterial and venous thrombotic events, and less severe COVID-19.
Copyright © 2022 Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosures The authors have no conflicts of interest to declare.
Figures
References
-
- DeLago AJ, Essa M, Ghajar A, Hammond-Haley M, Parvez A, Nawaz I, Shalhoub J, Marshall DC, Nazarian S, Calkins H, Salciccioli JD, Philips B. Incidence and mortality trends of atrial fibrillation/atrial flutter in the United States 1990 to 2017. Am J Cardiol. 2021;148:78–83. - PubMed
-
- Olesen JB, Lip GY, Hansen ML, Hansen PR, Tolstrup JS, Lindhardsen J, Selmer C, Ahlehoff O, Olsen AM, Gislason GH. Torp-Pedersen C. Validation of risk stratification schemes for predicting stroke and thromboembolism in patients with atrial fibrillation: nationwide cohort study. BMJ. 2011;342:d124. - PMC - PubMed
-
- Patel MR, Mahaffey KW, Garg J, Pan G, Singer DE, Hacke W, Breithardt G, Halperin JL, Hankey GJ, Piccini JP, Becker RC, Nessel CC, Paolini JF, Berkowitz SD, Fox KA, Califf RM, ROCKET AF Investigators Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011;365:883–891. - PubMed
-
- Granger CB, Alexander JH, McMurray JJ, Lopes RD, Hylek EM, Hanna M, Al-Khalidi HR, Ansell J, Atar D, Avezum A, Bahit MC, Diaz R, Easton JD, Ezekowitz JA, Flaker G, Garcia D, Geraldes M, Gersh BJ, Golitsyn S, Goto S, Hermosillo AG, Hohnloser SH, Horowitz J, Mohan P, Jansky P, Lewis BS, Lopez-Sendon JL, Pais P, Parkhomenko A, Verheugt FW, Zhu J, Wallentin L, ARISTOTLE Committees and Investigators Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365:981–992. - PubMed
-
- Connolly SJ, Ezekowitz MD, Yusuf S, Eikelboom J, Oldgren J, Parekh A, Pogue J, Reilly PA, Themeles E, Varrone J, Wang S, Alings M, Xavier D, Zhu J, Diaz R, Lewis BS, Darius H, Diener HC, Joyner CD, Wallentin L. RE-LY Steering Committee and Investigators. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361:1139–1151. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
