

Molecular epidemiology of enteroviruses associated with hand, foot, and mouth disease in South India from 2015 to 2017
- PMID: 35970888
- PMCID: PMC9377658
- DOI: 10.1007/s00705-022-05561-0
Molecular epidemiology of enteroviruses associated with hand, foot, and mouth disease in South India from 2015 to 2017
Abstract
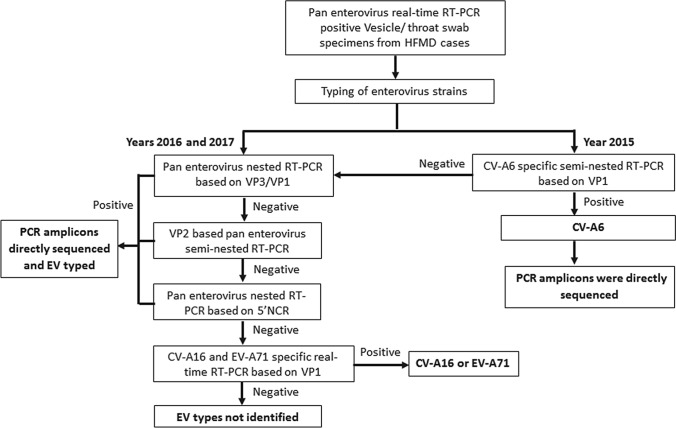
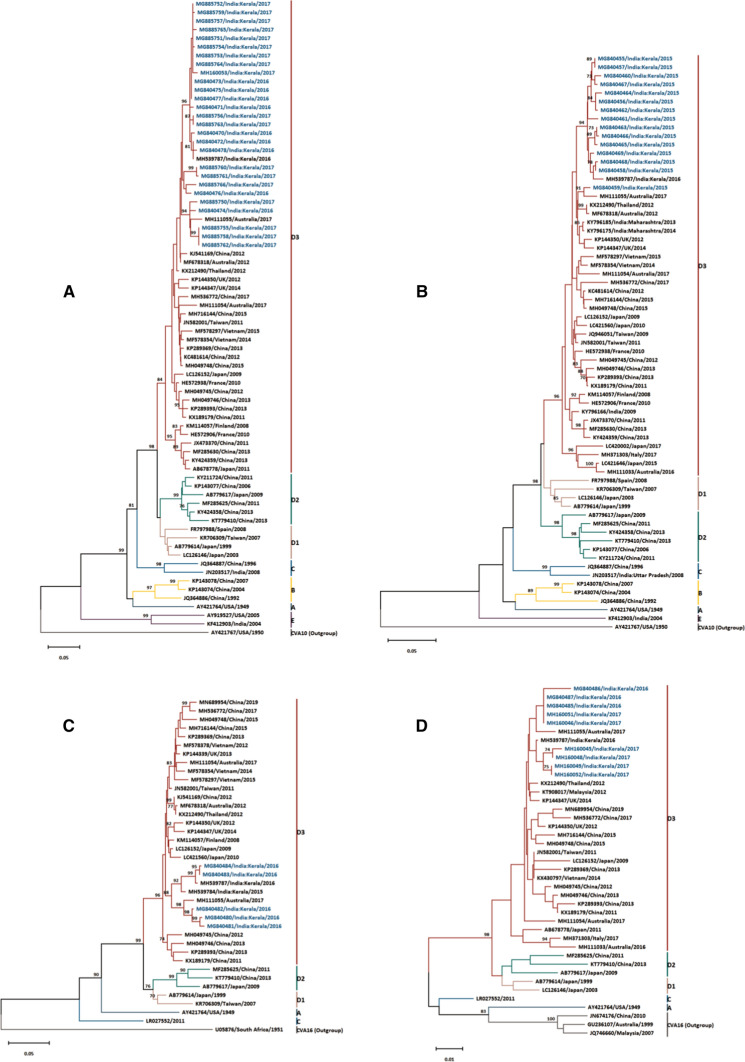
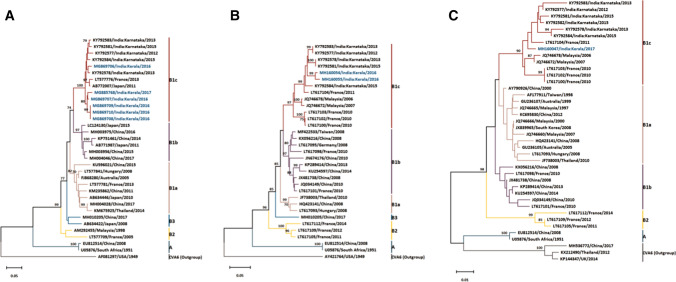
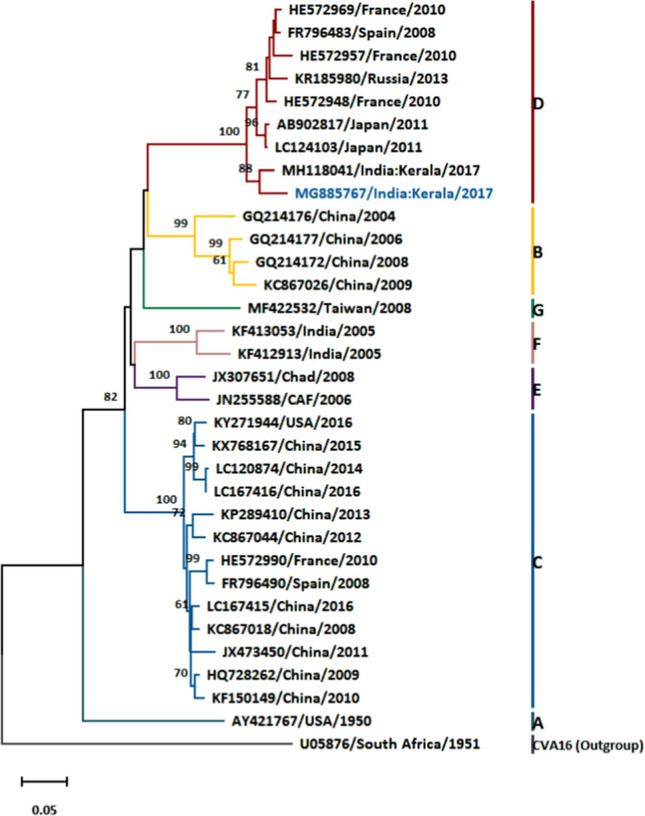
Hand, foot, and mouth disease (HFMD) is a common childhood infection caused by human enteroviruses and is clinically characterised by fever with vesicular rash on the hands, feet, and mouth. While enterovirus A71 (EV-A71) and coxsackievirus A16 (CVA16) were the major etiological agents of HFMD in India earlier, the data on recently circulating enteroviruses associated with HFMD are sparse. Here, we describe the molecular epidemiology of enteroviruses associated with HFMD in South India from 2015 to 2017. We used archived enterovirus real-time reverse transcription (RT) PCR-positive vesicle swab and/or throat swab specimens from clinically suspected HFMD cases collected from four secondary-care hospitals in South India between July 2015 and December 2017. PCR amplification and sequencing were done based on the 5'VP1, 3'VP1, VP2, or 5´NCR regions to identify enterovirus types. Genetic diversity among enteroviruses was inferred by phylogenetic analysis. Of the 107 enterovirus RNA real-time RT-PCR-positive HFMD cases, 69 (64%) were typed as CVA6, 16 (15%) were CVA16, and one (1%) was CVA10, whereas in 21 (20%) cases, the virus was not typeable by any of the methods used in the study. The majority of HFMD cases (89, 83%) were in children less than five years old, while 11 (10.3%) were in adults. 5'VP1 yielded the maximum number of enteroviruses genotyped, and phylogenetic analysis showed that the CVA6 strains belonged to subclade D3, while the subclades of CVA16 and CVA10 were B1c and D, respectively. The predominant etiological agent of HFMD in South India during 2015-2017 was CVA6, followed by CVA16 and CVA10.
© 2022. The Author(s), under exclusive licence to Springer-Verlag GmbH Austria, part of Springer Nature.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

Similar articles
-
Genetic characterization of enterovirus strains identified in Hand, Foot and Mouth Disease (HFMD): Emergence of B1c, C1 subgenotypes, E2 sublineage of CVA16, EV71 and CVA6 strains in India.Infect Genet Evol. 2017 Oct;54:192-199. doi: 10.1016/j.meegid.2017.05.024. Epub 2017 Jun 1. Infect Genet Evol. 2017. PMID: 28577914
-
Etiology of Multiple Non-EV71 and Non-CVA16 Enteroviruses Associated with Hand, Foot and Mouth Disease in Jinan, China, 2009-June 2013.PLoS One. 2015 Nov 12;10(11):e0142733. doi: 10.1371/journal.pone.0142733. eCollection 2015. PLoS One. 2015. PMID: 26562154 Free PMC article.
-
Epidemiological and molecular characteristics of circulating CVA16, CVA6 strains and genotype distribution in hand, foot and mouth disease cases in 2017 to 2018 from Western India.J Med Virol. 2021 Jun;93(6):3572-3580. doi: 10.1002/jmv.26454. Epub 2020 Oct 1. J Med Virol. 2021. PMID: 32833231
-
Atypical hand-foot-mouth disease in Belém, Amazon region, northern Brazil, with detection of coxsackievirus A6.J Clin Virol. 2020 May;126:104307. doi: 10.1016/j.jcv.2020.104307. Epub 2020 Mar 6. J Clin Virol. 2020. PMID: 32302950 Review.
-
Potential therapeutic substances for hand-foot-and-mouth disease in the interplay of enteroviruses and type I interferon.Int J Antimicrob Agents. 2025 May;65(5):107464. doi: 10.1016/j.ijantimicag.2025.107464. Epub 2025 Feb 15. Int J Antimicrob Agents. 2025. PMID: 39956531 Review.
Cited by
-
Molecular Epidemiology and Evolution of Coxsackievirus A14.Viruses. 2023 Nov 26;15(12):2323. doi: 10.3390/v15122323. Viruses. 2023. PMID: 38140564 Free PMC article.
-
'Tomato flu' a new epidemic in India: Virology, epidemiology, and clinical features.New Microbes New Infect. 2022 Dec 13;51:101070. doi: 10.1016/j.nmni.2022.101070. eCollection 2023 Jan. New Microbes New Infect. 2022. PMID: 36582550 Free PMC article. Review.
-
Emergence of Recombinant Subclade D3/Y in Coxsackievirus A6 Strains in Hand-Foot-and-Mouth Disease (HFMD) Outbreak in India, 2022.Microorganisms. 2024 Feb 28;12(3):490. doi: 10.3390/microorganisms12030490. Microorganisms. 2024. PMID: 38543541 Free PMC article.
-
Genomic surveillance reveals low-level circulation of two subtypes of genogroup C coxsackievirus A10 in Nanchang, Jiangxi Province, China, 2015-2023.Front Microbiol. 2024 Sep 17;15:1459917. doi: 10.3389/fmicb.2024.1459917. eCollection 2024. Front Microbiol. 2024. PMID: 39355427 Free PMC article.
-
First Report of Hand, Foot, and Mouth Disease (HFMD) Outbreak in the West Bank, Palestine: Molecular Characterization of Coxsackievirus A16 (CV-A16).Can J Infect Dis Med Microbiol. 2025 Feb 18;2025:9133821. doi: 10.1155/cjid/9133821. eCollection 2025. Can J Infect Dis Med Microbiol. 2025. PMID: 40007683 Free PMC article.
References
-
- Pacific WHORO for the W. A guide to clinical management and public health response for hand, foot and mouth disease (HFMD) [Internet]. Manila : WHO Regional Office for the Western Pacific; 2011. https://iris.wpro.who.int/handle/10665.1/5521. Accessed 24 May 2020
-
- Identification and molecular characterization of non-polio enteroviruses from children with acute flaccid paralysis in West Africa, 2013–2014 [Internet]. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5476622/. Accessed 29 May 2019 - PMC - PubMed
-
- Kim B, Moon S, Bae GR, Lee H, Pai H, Oh SH. Factors associated with severe neurologic complications in patients with either hand-foot-mouth disease or herpangina: a nationwide observational study in South Korea, 2009–2014. Lau EHY, editor. PLoS ONE. 2018;13(8):e0201726. doi: 10.1371/journal.pone.0201726. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
