

Use of Covered Stents in Cannulation Sites as a Last Option to Salvage Failing Vascular Access
- PMID: 35972139
- PMCID: PMC10773153
- DOI: 10.1177/15266028221116745
Use of Covered Stents in Cannulation Sites as a Last Option to Salvage Failing Vascular Access
Abstract
Purpose: Controversy exists regarding the treatment of recurrent stenosis in vascular access at cannulation sites with a covered stent as repeated cannulation may damage the stent. The purpose of this study was to review covered stent placement at cannulation sites to salvage failing vascular access.
Materials and methods: A total of 11 patients were included for the purpose of this study. Eight patients (72.7%) received a covered stent due to recurrent stenosis, 2 (18.2%) due to an acute occlusion, and in 1 case (9.1%), the covered stent was used to repair a damaged polytetrafluoroethylene arteriovenous graft (PTFE AVG).
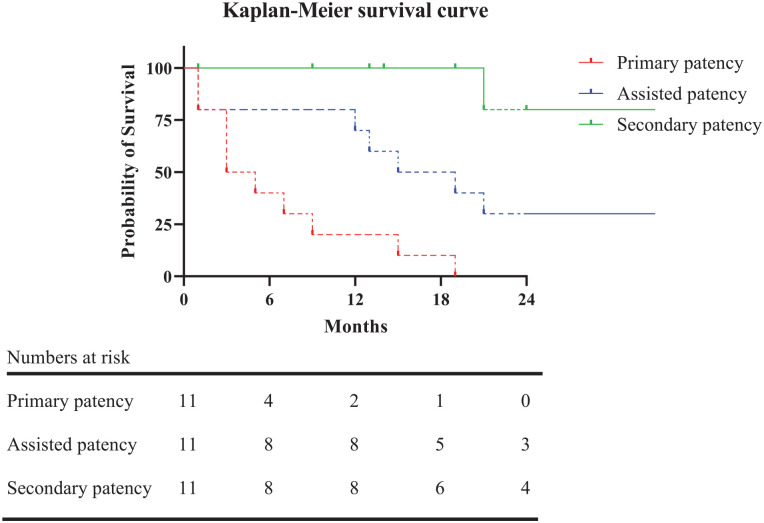
Results: Primary patency after stent placement was 40.9% at 6 months, primary-assisted patency was 79.5% at 12 months, and secondary patency was 80% at 24 months. No significant problems were observed during the dialysis sessions after stent placement. The intervention rate per patient-year was not significantly different before or after covered stent placement, at 3.8 (IQR=9.5) interventions per year versus 2.5 (IQR=3.0) interventions per year (p=0.280).
Conclusion: In conclusion, treating failing vascular access with problems at cannulation sites with covered stents can be considered.
Clinical impact: Treating vascular access stenosis at cannulation sites with covered stents can successfully prolong vascular access life.
Keywords: covered stent graft; endovascular treatment/therapy; hemodialysis; puncture; vascular access.
Conflict of interest statement
Declaration of Conflicting InterestsThe author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures

Similar articles
-
Postintervention Patency: A Comparison of Stenting versus Patch Angioplasty for Dysfunctional Hemodialysis Access Sites.Ann Vasc Surg. 2016 May;33:120-5. doi: 10.1016/j.avsg.2015.12.004. Epub 2016 Mar 8. Ann Vasc Surg. 2016. PMID: 26965804
-
Evaluating patency rates of an ultralow-porosity expanded polytetrafluoroethylene covered stent in the treatment of venous stenosis in arteriovenous dialysis circuits.J Vasc Interv Radiol. 2014 Feb;25(2):183-9. doi: 10.1016/j.jvir.2013.10.006. Epub 2013 Nov 25. J Vasc Interv Radiol. 2014. PMID: 24286940
-
Safety and efficacy of a new covered stent in hemodialysis vascular access outflow stenosis: A Brazilian multicenter retrospective study.J Vasc Access. 2025 Mar;26(2):510-518. doi: 10.1177/11297298231226259. Epub 2024 Feb 5. J Vasc Access. 2025. PMID: 38316624 Free PMC article.
-
The role of stents in hemodialysis vascular access.J Vasc Access. 2023 Jan;24(1):107-116. doi: 10.1177/11297298211015069. Epub 2021 May 17. J Vasc Access. 2023. PMID: 33993804 Free PMC article. Review.
-
Stent grafts for treatment of cannulation zone stenosis and arteriovenous graft venous anastomosis.J Vasc Access. 2017 Mar 6;18(Suppl. 1):47-52. doi: 10.5301/jva.5000680. Epub 2017 Mar 5. J Vasc Access. 2017. PMID: 28297058 Review.
Cited by
-
The case against stenting the cannulation zone of dialysis access.Radiol Case Rep. 2024 Sep 16;19(12):5893-5895. doi: 10.1016/j.radcr.2024.08.141. eCollection 2024 Dec. Radiol Case Rep. 2024. PMID: 39319171 Free PMC article.
-
Hemodialysis Access Stent Graft Trials: Past, Present, and Future.Cardiovasc Intervent Radiol. 2023 Sep;46(9):1154-1161. doi: 10.1007/s00270-023-03389-y. Epub 2023 Mar 20. Cardiovasc Intervent Radiol. 2023. PMID: 36941431 Review. No abstract available.
References
-
- Vascular Access Work Group. Clinical practice guidelines for vascular access. Am J Kidney Dis. 2006;48(suppl 1):248. - PubMed
-
- Haskal ZJ, Saad TF, Hoggard JG, et al. Prospective, randomized, concurrently-controlled study of a stent graft versus balloon angioplasty for treatment of arteriovenous access graft stenosis: 2-year results of the RENOVA study. J Vasc Interv Radiol. 2016;27(8):1105–1114. doi: 10.1016/j.jvir.2016.05.019. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
