

Temporal Changes in Cholangiocarcinoma Incidence and Mortality in the United States from 2001 to 2017
- PMID: 35972334
- PMCID: PMC9526482
- DOI: 10.1093/oncolo/oyac150
Temporal Changes in Cholangiocarcinoma Incidence and Mortality in the United States from 2001 to 2017
Abstract
Background: Previous studies report increasing cholangiocarcinoma (CCA) incidence up to 2015. This contemporary retrospective analysis of CCA incidence and mortality in the US from 2001-2017 assessed whether CCA incidence continued to increase beyond 2015.
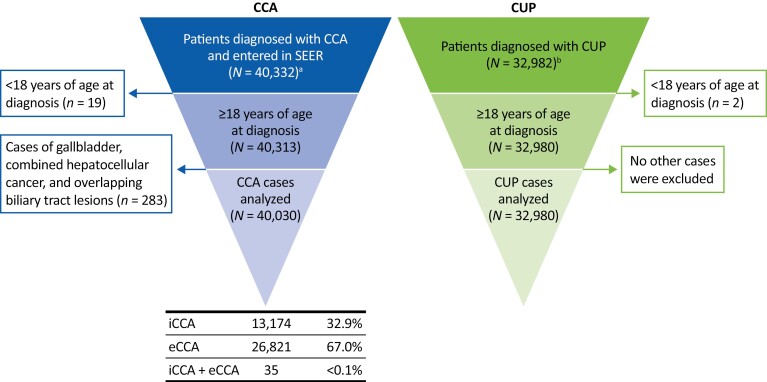
Patients and methods: Patients (≥18 years) with CCA were identified in the National Cancer Institute Surveillance, Epidemiology, and End Results 18 cancer registry (International Classification of Disease for Oncology [ICD-O]-3 codes: intrahepatic [iCCA], C221; extrahepatic [eCCA], C240, C241, C249). Cancer of unknown primary (CUP) cases were identified (ICD-O-3: C809; 8140/2, 8140/3, 8141/3, 8143/3, 8147/3) because of potential misclassification as iCCA.
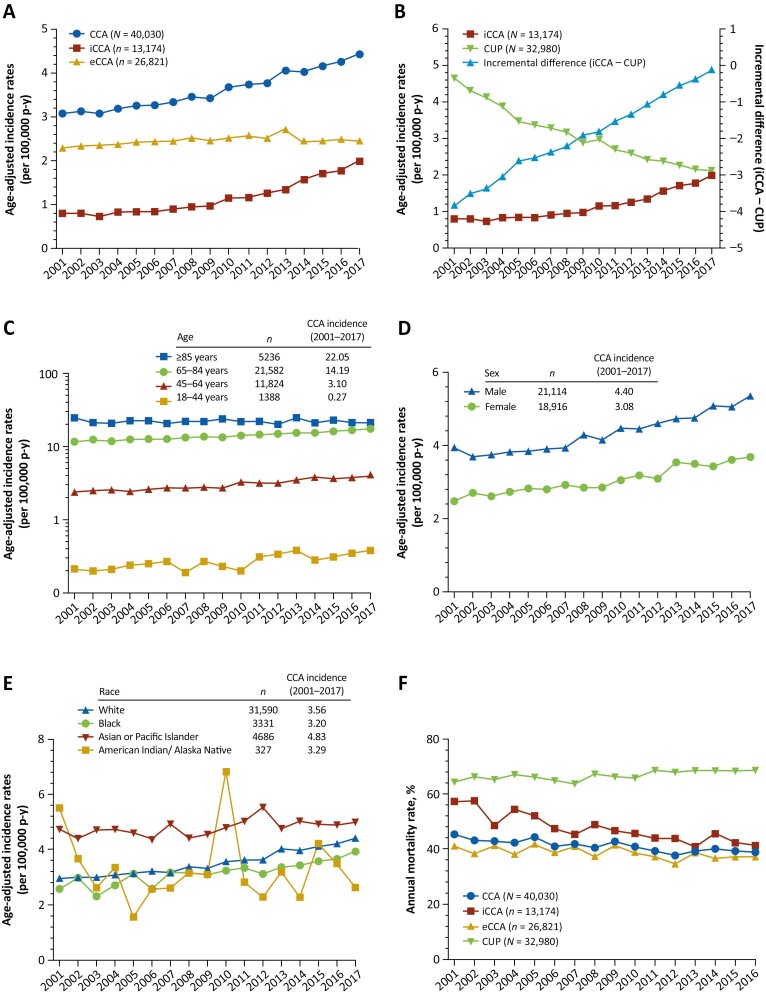
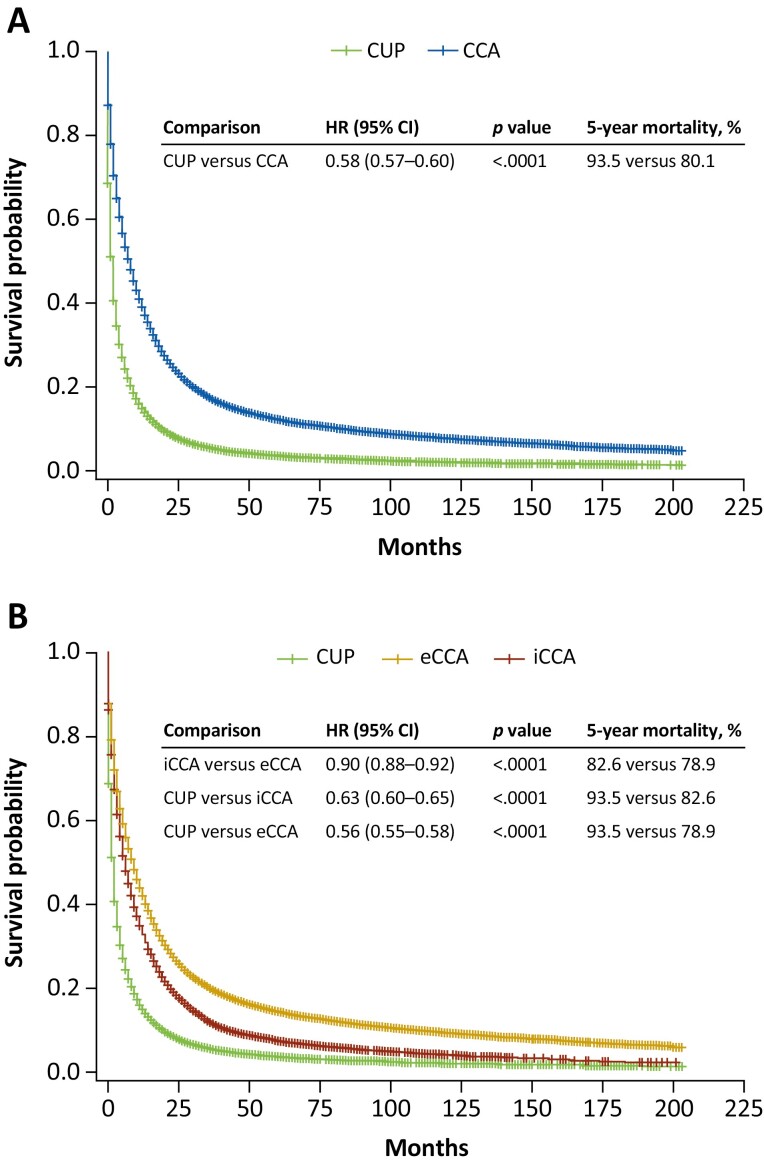
Results: Forty-thousand-and-thirty CCA cases (iCCA, n=13,174; eCCA, n=26,821; iCCA and eCCA, n=35) and 32,980 CUP cases were analyzed. From 2001-2017, CCA, iCCA, and eCCA incidence (per 100 000 person-years) increased 43.8% (3.08 to 4.43), 148.8% (0.80 to 1.99), and 7.5% (2.28 to 2.45), respectively. In contrast, CUP incidence decreased 54.4% (4.65 to 2.12). CCA incidence increased with age, with greatest increase among younger patients (18-44 years, 81.0%). Median overall survival from diagnosis was 8, 6, 9, and 2 months for CCA, iCCA, eCCA, and CUP. From 2001-2016, annual mortality rate declined for iCCA (57.1% to 41.2%) and generally remained stable for eCCA (40.9% to 37.0%) and for CUP (64.3% to 68.6%).
Conclusions: CCA incidence continued to increase from 2001-2017, with greater increase in iCCA versus eCCA, whereas CUP incidence decreased. The divergent CUP versus iCCA incidence trends, with overall greater absolute change in iCCA incidence, provide evidence for a true increase in iCCA incidence that may not be wholly attributable to CUP reclassification.
Keywords: SEER program; cholangiocarcinoma; incidence; mortality; prevalence; unknown primary tumor.
© The Author(s) 2022. Published by Oxford University Press.
Figures
References
-
- Varadhachary GR, Raber MN.. Cancer of unknown primary site. N Engl J Med. 2014;371(8):757-765. 10.1056/NEJMra1303917. https://www.nejm.org/doi/10.1056/NEJMra1303917 - DOI - PubMed
