

Pancreatic Cancer Patient-derived Organoids Can Predict Response to Neoadjuvant Chemotherapy
- PMID: 35972511
- PMCID: PMC10202108
- DOI: 10.1097/SLA.0000000000005558
Pancreatic Cancer Patient-derived Organoids Can Predict Response to Neoadjuvant Chemotherapy
Abstract
Objective: To evaluate if patient-derived organoids (PDOs) may predict response to neoadjuvant (NAT) chemotherapy in patients with pancreatic adenocarcinoma.
Background: PDOs have been explored as a biomarker of therapy response and for personalized therapeutics in patients with pancreatic cancer.
Methods: During 2017-2021, patients were enrolled into an IRB-approved protocol and PDO cultures were established. PDOs of interest were analyzed through a translational pipeline incorporating molecular profiling and drug sensitivity testing.
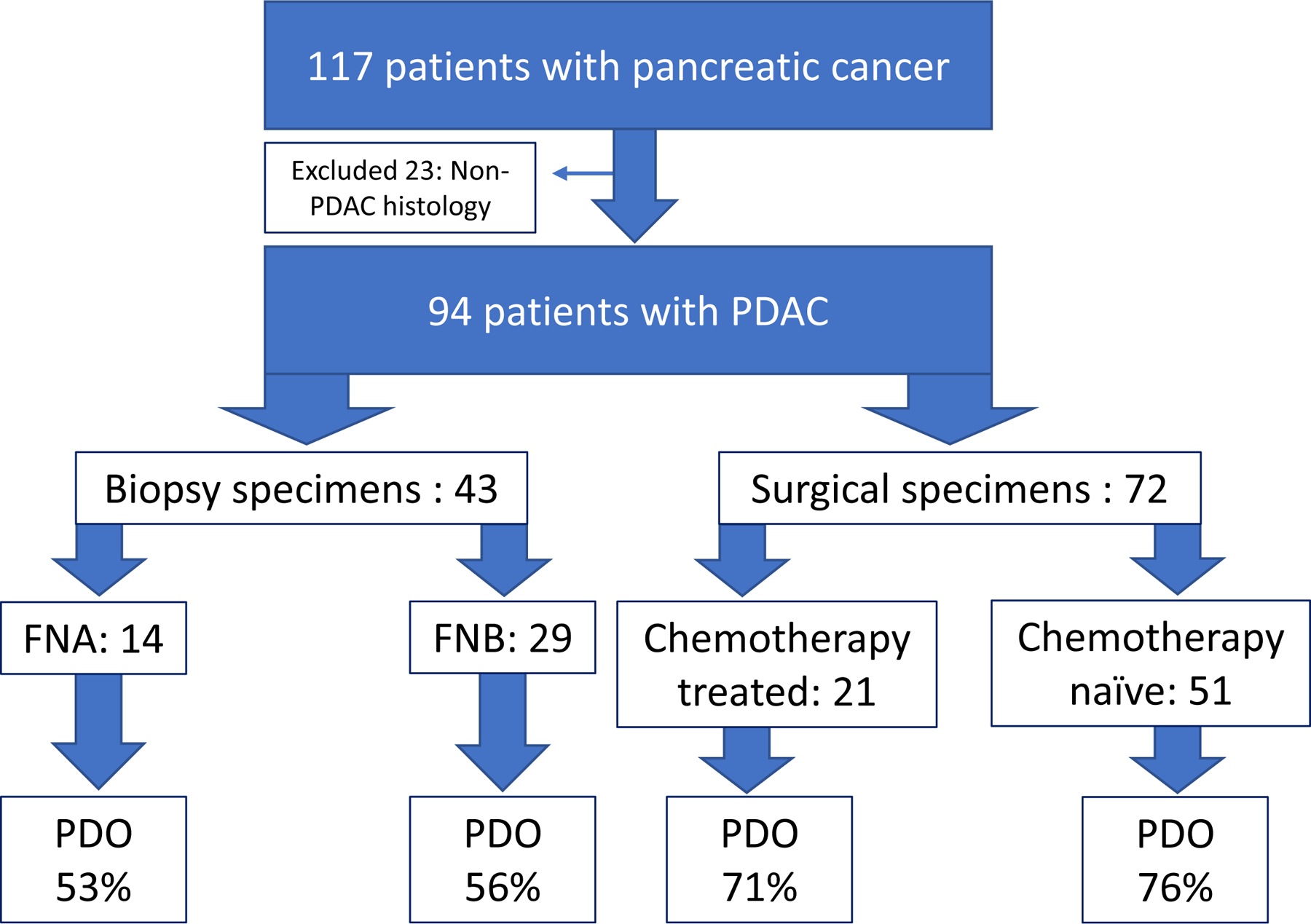
Results: One hundred thirty-six samples, including both surgical resections and fine needle aspiration/biopsy from 117 patients with pancreatic cancer were collected. This biobank included diversity in stage, sex, age, and race, with minority populations representing 1/3 of collected cases (16% Black, 9% Asian, 7% Hispanic/Latino). Among surgical specimens, PDO generation was successful in 71% (15 of 21) of patients who had received NAT prior to sample collection and in 76% (39 of 51) of patients who were untreated with chemotherapy or radiation at the time of collection. Pathological response to NAT correlated with PDO chemotherapy response, particularly oxaliplatin. We demonstrated the feasibility of a rapid PDO drug screen and generated data within 7 days of tissue resection.
Conclusion: Herein we report a large single-institution organoid biobank, including ethnic minority samples. The ability to establish PDOs from chemotherapy-naive and post-NAT tissue enables longitudinal PDO generation to assess dynamic chemotherapy sensitivity profiling. PDOs can be rapidly screened and further development of rapid screening may aid in the initial stratification of patients to the most active NAT regimen.
Copyright © 2022 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors report no conflicts of interest.
Figures






References
-
- Tempero MA, Malafa MP, Al-Hawary M, et al. Pancreatic Adenocarcinoma, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw 2021;19(4):439–457. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
