Extent of Tumor Resection and Survival in Pediatric Patients With High-Grade Gliomas: A Systematic Review and Meta-analysis
- PMID: 35972743
- PMCID: PMC9382445
- DOI: 10.1001/jamanetworkopen.2022.26551
Extent of Tumor Resection and Survival in Pediatric Patients With High-Grade Gliomas: A Systematic Review and Meta-analysis
Abstract
Importance: Pediatric patients with high-grade gliomas have a poor prognosis. The association among the extent of resection, tumor location, and survival in these patients remains unclear.
Objective: To ascertain whether gross total resection (GTR) in hemispheric, midline, or infratentorial pediatric high-grade gliomas (pHGGs) is independently associated with survival differences compared with subtotal resection (STR) and biopsy at 1 year and 2 years after tumor resection.
Data sources: PubMed, EBMR, Embase, and MEDLINE were systematically reviewed from inception to June 3, 2022, using the keywords high-grade glioma, pediatric, and surgery. No period or language restrictions were applied.
Study selection: Randomized clinical trials and cohort studies of pHGGs that stratified patients by extent of resection and reported postoperative survival were included for study-level and individual patient data meta-analyses.
Data extraction and synthesis: Study characteristics and mortality rates were extracted from each article. Relative risk ratios (RRs) were pooled using random-effects models. Individual patient data were evaluated using multivariate mixed-effects Cox proportional hazards regression modeling. The PRISMA reporting guideline was followed, and the study was registered a priori.
Main outcomes and measures: Hazard ratios (HRs) and RRs were extracted to indicate associations among extent of resection, 1-year and 2-year postoperative mortality, and overall survival.
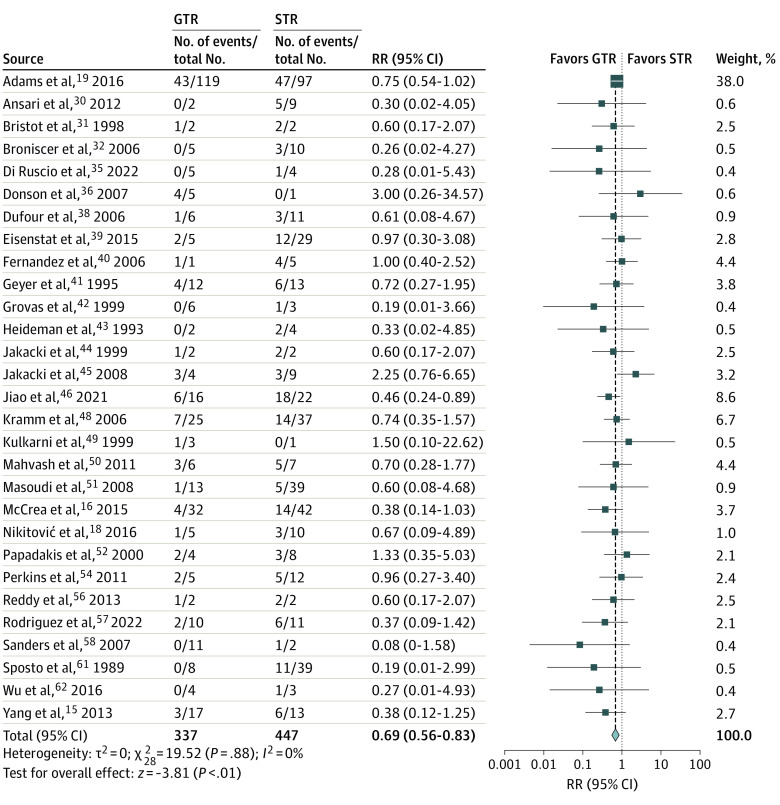
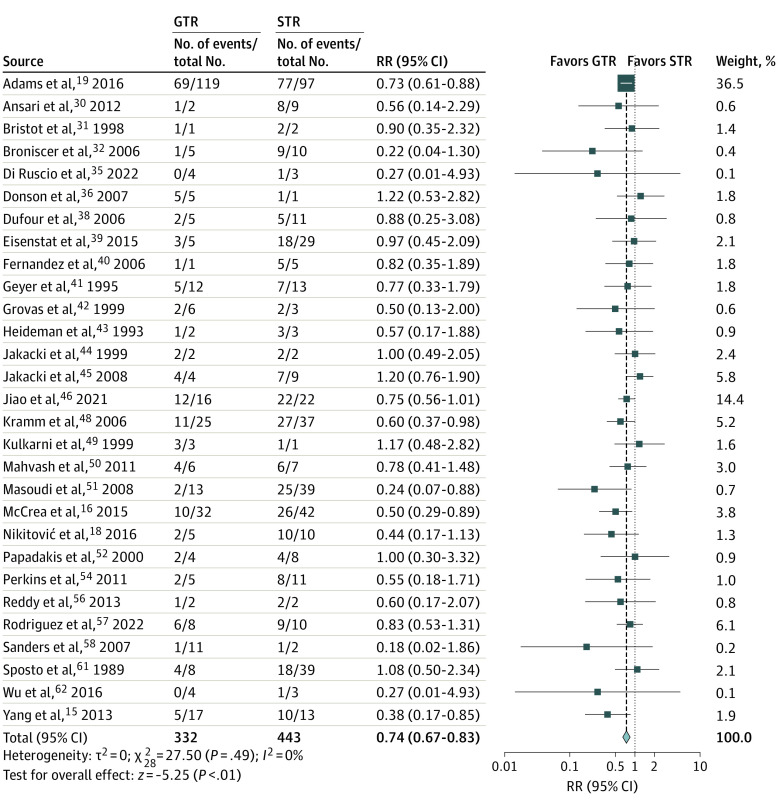
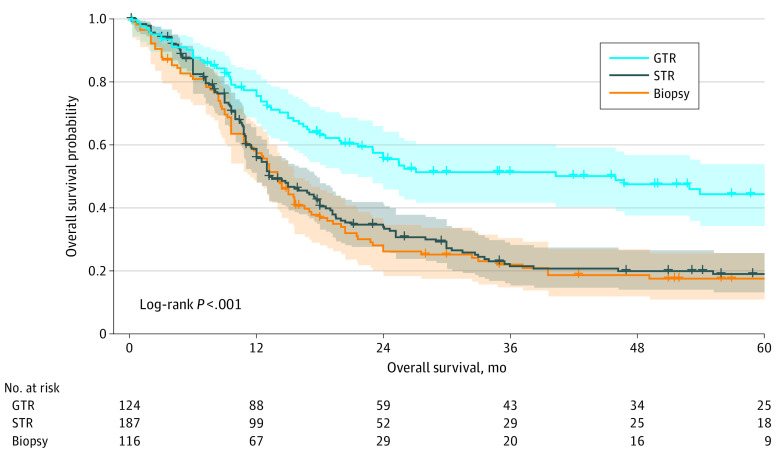
Results: A total of 37 studies with 1387 unique patients with pHGGs were included. In study-level meta-analysis, GTR had a lower mortality risk than STR at 1 year (RR, 0.69; 95% CI, 0.56-0.83; P < .001) and 2 years (RR, 0.74; 95% CI, 0.67-0.83; P < .001) after tumor resection. Subtotal resection was not associated with differential survival compared with biopsy at 1 year (RR, 0.82; 95% CI, 0.66-1.01; P = .07) but had decreased mortality risk at 2 years (RR, 0.89; 95% CI, 0.82-0.97; P = .01). The individual patient data meta-analysis of 27 articles included 427 patients (mean [SD] age at diagnosis, 9.3 [5.9] years), most of whom were boys (169 of 317 [53.3%]), had grade IV tumors (246 of 427 [57.7%]), and/or had tumors that were localized to either the cerebral hemispheres (133 of 349 [38.1%]) or midline structures (132 of 349 [37.8%]). In the multivariate Cox proportional hazards regression model, STR (HR, 1.91; 95% CI, 1.34-2.74; P < .001) and biopsy (HR, 2.10; 95% CI, 1.43-3.07; P < .001) had shortened overall survival compared with GTR but no survival differences between them (HR, 0.91; 95% CI, 0.67-1.24; P = .56). Gross total resection was associated with prolonged survival compared with STR for hemispheric (HR, 0.29; 95% CI, 0.15-0.54; P < .001) and infratentorial (HR, 0.44; 95% CI, 0.24-0.83; P = .01) tumors but not midline tumors (HR, 0.63; 95% CI, 0.34-1.19; P = .16).
Conclusions and relevance: Results of this study show that, among patients with pHGG, GTR is independently associated with better overall survival compared with STR and biopsy, especially among patients with hemispheric and infratentorial tumors, and support the pursuit of maximal safe resection in the treatment of pHGGs.
Conflict of interest statement
Figures