

Cardiovascular and Renal Implications of Myocardial Infarction in the ISCHEMIA-CKD Trial
- PMID: 35973009
- PMCID: PMC10865178
- DOI: 10.1161/CIRCINTERVENTIONS.122.012103
Cardiovascular and Renal Implications of Myocardial Infarction in the ISCHEMIA-CKD Trial
Abstract
Background: ISCHEMIA-CKD (International Study of Comparative Health Effectiveness With Medical and Invasive Approaches-Chronic Kidney Disease) reported an initial invasive treatment strategy did not reduce the risk of death or nonfatal myocardial infarction (MI) compared with a conservative treatment strategy in patients with advanced chronic kidney disease, stable coronary disease, and moderate or severe myocardial ischemia. The cumulative frequency of different MI type after randomization and subsequent prognosis have not been reported.
Methods: MI classification was based on the Third Universal Definition for MI. For procedural MI, the primary MI definition used creatine kinase-MB as the preferred biomarker, whereas the secondary MI definition used cTn (cardiac troponin); both definitions included elevated biomarker-only events with higher thresholds than nonprocedural MIs. The cumulative frequency of MI type according to treatment strategy was determined. The association of MI with subsequent all-cause death and new dialysis initiation was assessed by treating MI as a time-dependent covariate.
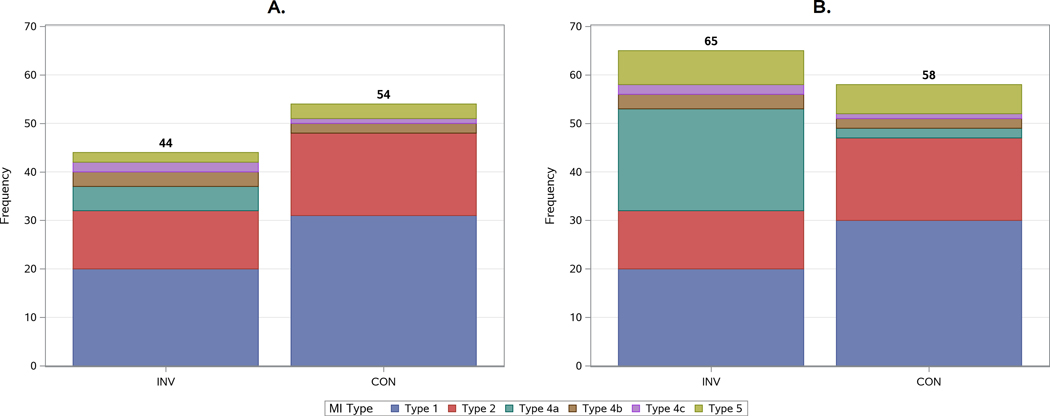
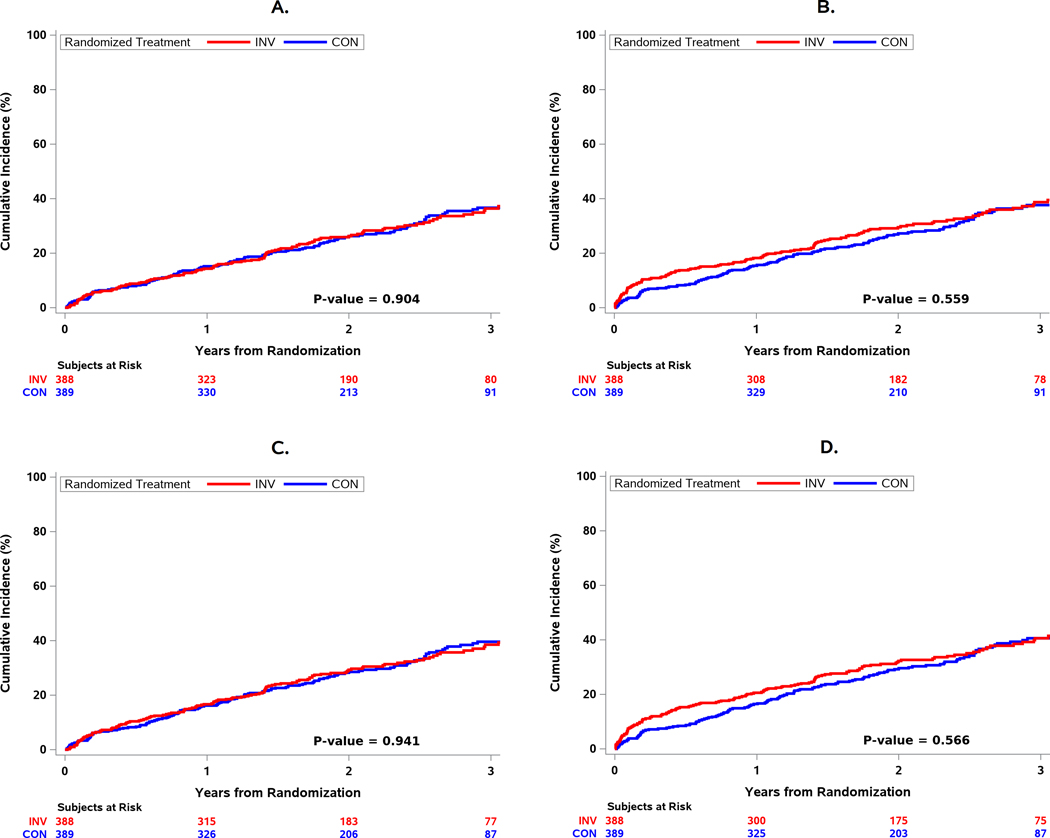
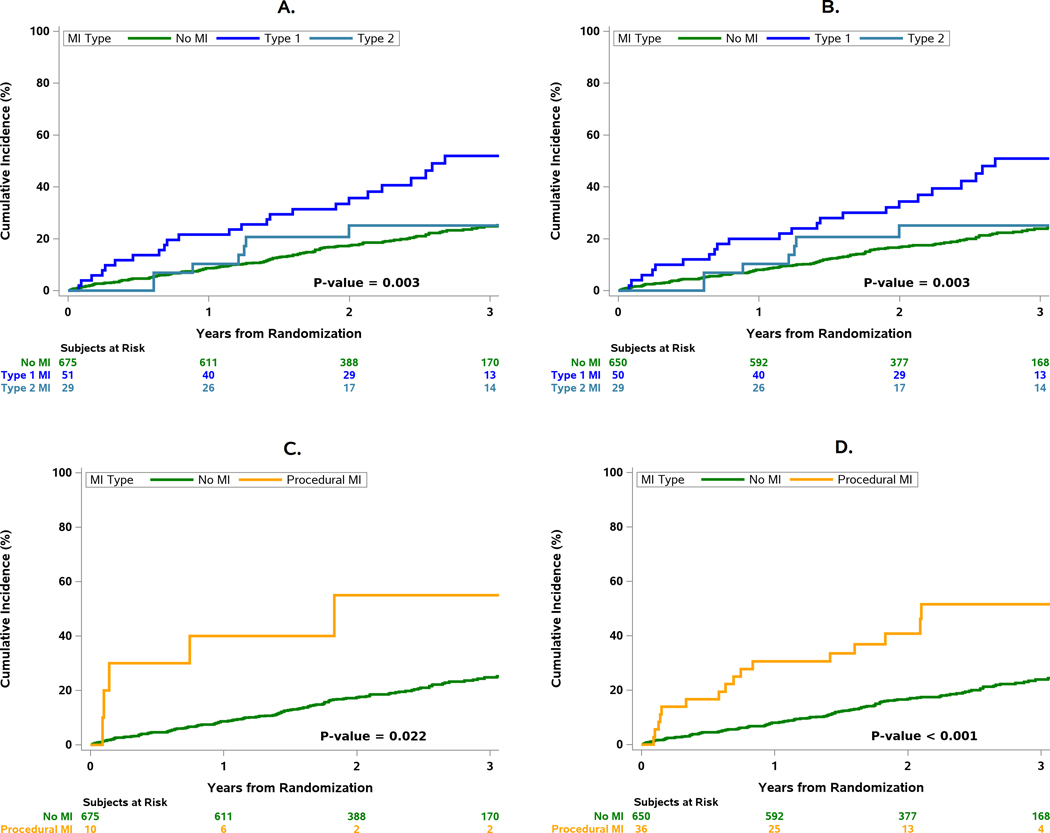
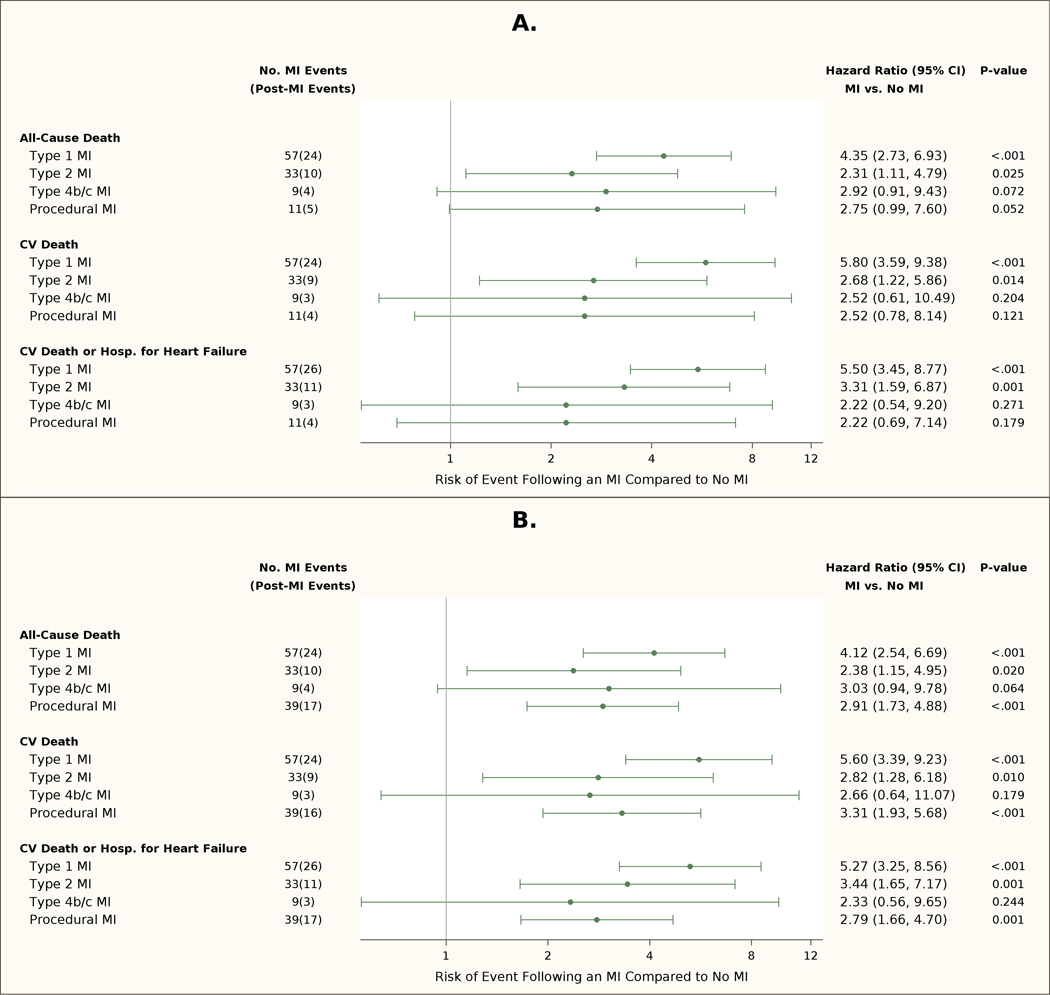
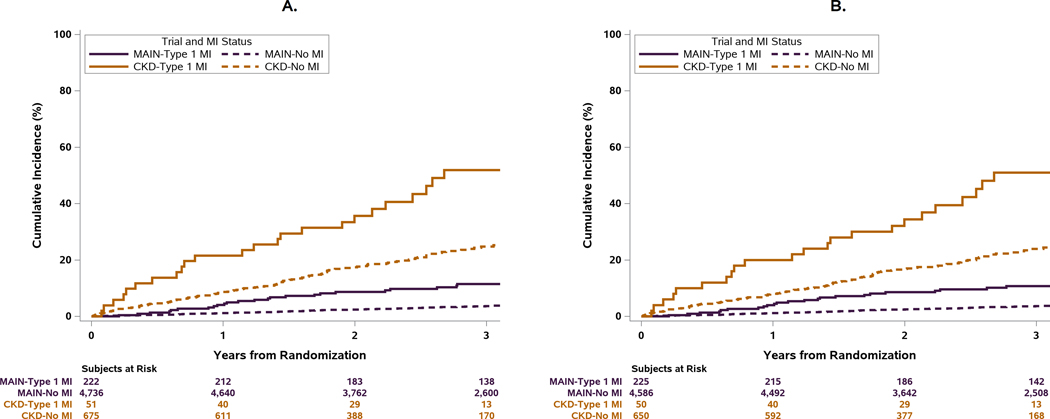
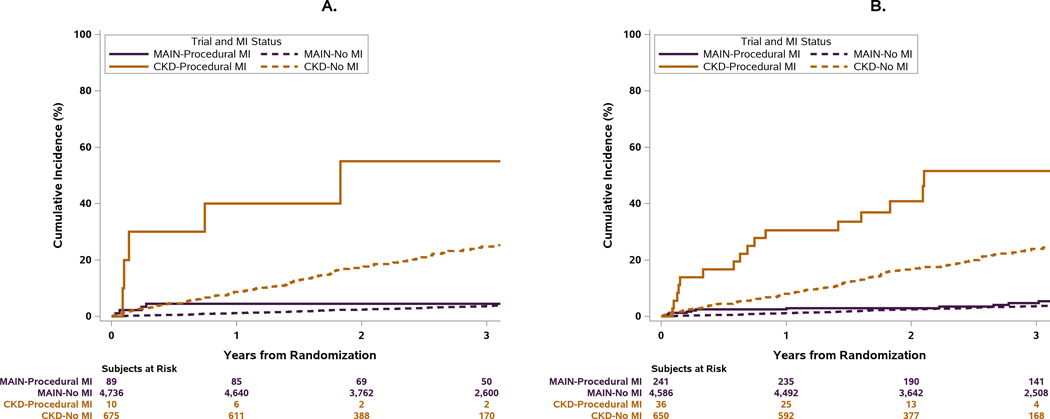
Results: The 3-year incidence of type 1 or 2 MI with the primary MI definition was 11.2% in invasive treatment strategy and 13.6% in conservative treatment strategy (hazard ratio [HR], 0.66 [95% CI, 0.42-1.02]). Procedural MIs were more frequent in invasive treatment strategy and accounted for 9.8% and 28.3% of all MIs with the primary and secondary MI definitions, respectively. Patients had an increased risk of all-cause death after type 1 MI (adjusted HR, 4.35 [95% CI, 2.73-6.93]) and after procedural MI with the primary (adjusted HR, 2.75 [95% CI, 0.99-7.60]) and secondary MI definitions (adjusted HR, 2.91 [95% CI, 1.73-4.88]). Dialysis initiation was increased after a type 1 MI (HR, 6.45 [95% CI, 2.59-16.08]) compared with patients without an MI.
Conclusions: In ISCHEMIA-CKD, the invasive treatment strategy had higher rates of procedural MIs, particularly with the secondary MI definition, and lower rates of type 1 and 2 MIs. Procedural MIs, type 1 MIs, and type 2 MIs were associated with increased risk of subsequent death. Type 1 MI increased the risk of dialysis initiation.
Registration: URL: https://www.
Clinicaltrials: gov; Unique identifier: NCT01985360.
Keywords: epidemiology; mortality; myocardial infarction; myocardial ischemia; myocardial revascularization; renal insufficiency, chronic.
Figures
References
-
- Sarnak MJ, Amann K, Bangalore S, Cavalcante JL, Charytan DM, Craig JC, Gill JS, Hlatky MA, Jardine AG, Landmesser U, Newby LK, Herzog CA, Cheung M, Wheeler DC, Winkelmayer WC, Marwick TH and Conference P. Chronic Kidney Disease and Coronary Artery Disease: JACC State-of-the-Art Review. J Am Coll Cardiol. 2019;74:1823–1838. - PubMed
-
- Herzog CA, Ma JZ and Collins AJ. Poor long-term survival after acute myocardial infarction among patients on long-term dialysis. N Engl J Med. 1998;339:799–805. - PubMed
-
- Herzog CA, Littrell K, Arko C, Frederick PD and Blaney M. Clinical characteristics of dialysis patients with acute myocardial infarction in the United States: a collaborative project of the United States Renal Data System and the National Registry of Myocardial Infarction. Circulation. 2007;116:1465–72. - PubMed
-
- Szummer K, Lindhagen L, Evans M, Spaak J, Koul S, Akerblom A, Carrero JJ and Jernberg T. Treatments and Mortality Trends in Cases With and Without Dialysis Who Have an Acute Myocardial Infarction: An 18-Year Nationwide Experience. Circ Cardiovasc Qual Outcomes. 2019;12:e005879. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
