

Late effects in patients with mantle cell lymphoma treated with or without autologous stem cell transplantation
- PMID: 35973196
- PMCID: PMC10018432
- DOI: 10.1182/bloodadvances.2022007241
Late effects in patients with mantle cell lymphoma treated with or without autologous stem cell transplantation
Abstract
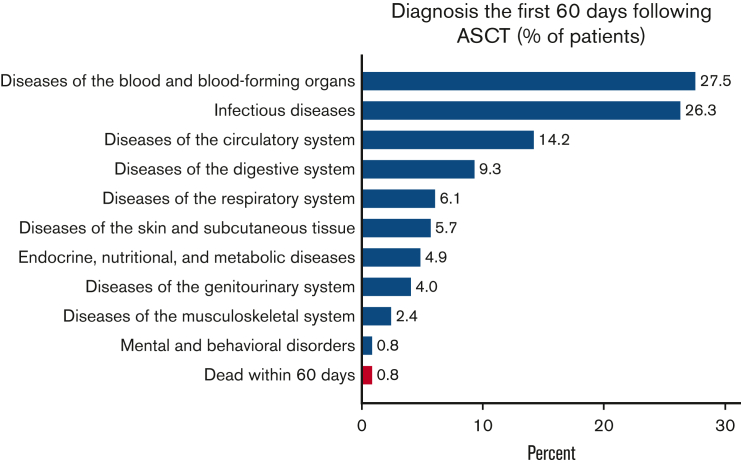
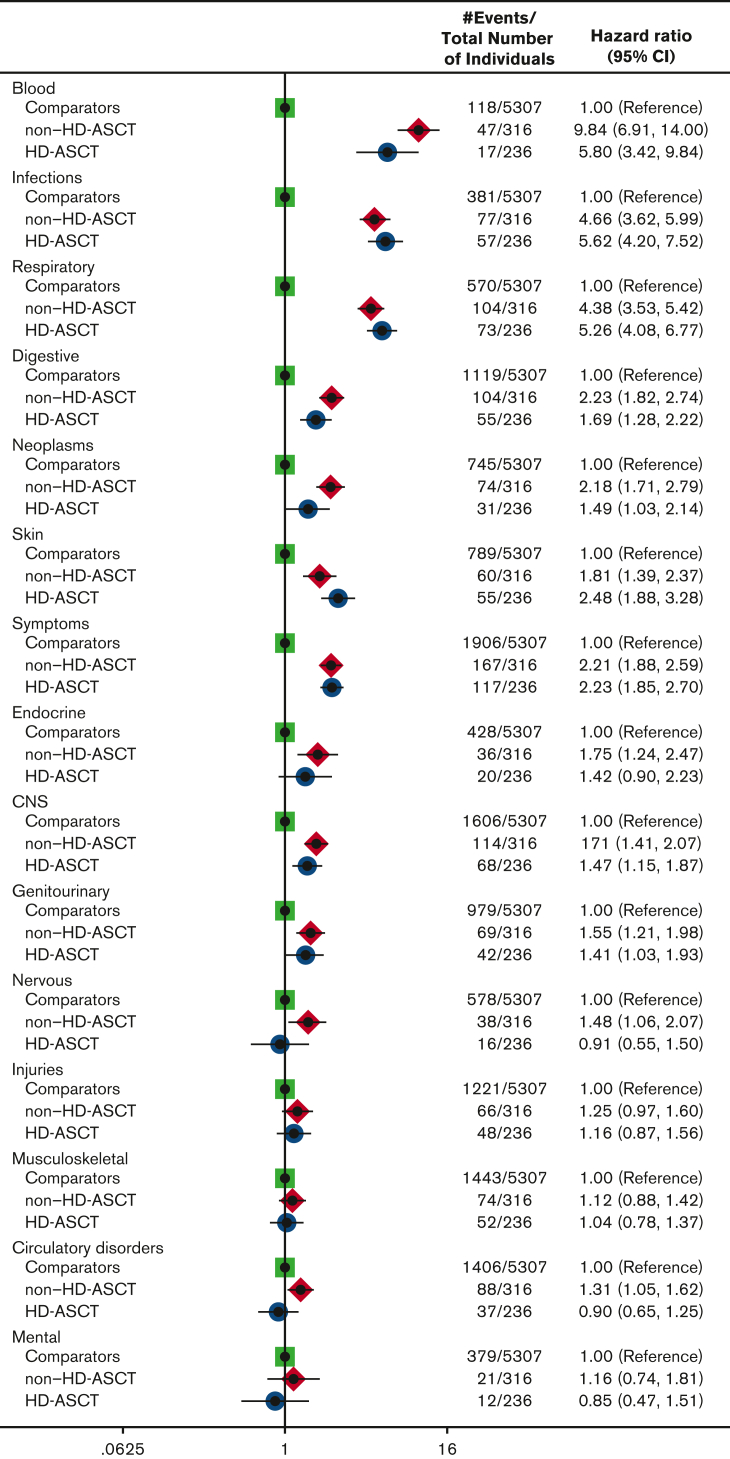
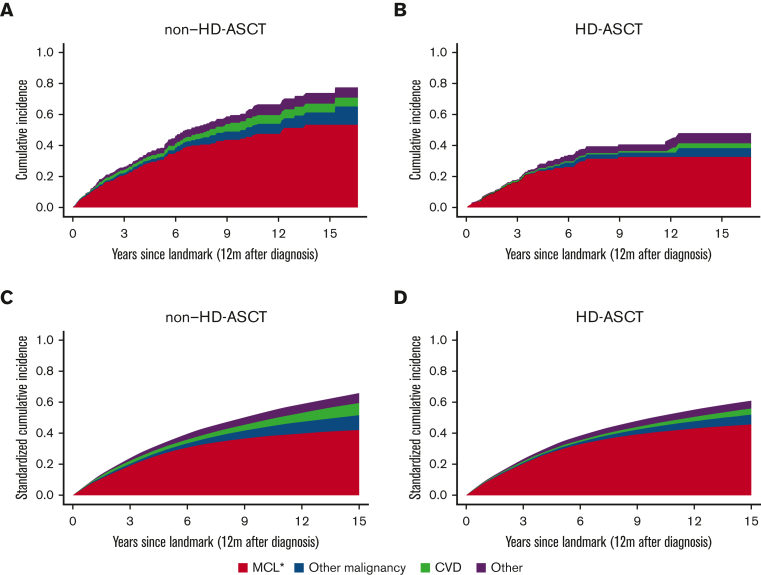
Studies on late effects in patients with mantle cell lymphoma (MCL) are becoming increasingly important as survival is improving, and novel targeted drugs are being introduced. However, knowledge about late effects is limited. The aim of this population-based study was to describe the magnitude and panorama of late effects among patients treated with or without high-dose chemotherapy with autologous stem cell transplantation (HD-ASCT). The study cohort included all patients with MCL, recorded in the Swedish Lymphoma Register, aged 18 to 69 years, diagnosed between 2000 and 2014 (N = 620; treated with HD-ASCT, n = 247) and 1:10 matched healthy comparators. Patients and comparators were followed up via the National Patient Register and Cause of Death Register, from 12 months after diagnosis or matching to December 2017. Incidence rate ratios of the numbers of outpatient visits, hospitalizations, and bed days were estimated using negative binomial regression models. In relation to the matched comparators, the rate of specialist and hospital visits was significantly higher among patients with MCL. Patients with MCL had especially high relative risks of infectious, respiratory, and blood disorders. Within this observation period, no difference in the rate of these complications, including secondary neoplasms, was observed between patients treated with and without HD-ASCT. Most of the patients died from their lymphoma and not from another cause or treatment complication. Taken together, our results imply that most of the posttreatment health care needs are related to the lymphoma disease itself, thus, indicating the need for more efficient treatment options.
© 2023 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: M.J. received honoraria from Janssen, Gilead, Celgene, Roche, and Acerta and research support from Janssen, Roche, Celgene, AbbVie, and Gilead. K.E.S. received honoraria from Celgene and research support from Janssen. I.G. received honoraria from Janssen. All authors participate in a public-private real-world evidence collaboration between Karolinska Institutet and Janssen Pharmaceuticals NV.
Figures
Similar articles
-
R-hyper-CVAD versus R-CHOP/cytarabine with high-dose therapy and autologous haematopoietic stem cell support in fit patients with mantle cell lymphoma: 20 years of single-center experience.Ann Hematol. 2018 Feb;97(2):277-287. doi: 10.1007/s00277-017-3180-x. Epub 2017 Nov 16. Ann Hematol. 2018. PMID: 29147847
-
Addition of high-dose cytarabine to immunochemotherapy before autologous stem-cell transplantation in patients aged 65 years or younger with mantle cell lymphoma (MCL Younger): a randomised, open-label, phase 3 trial of the European Mantle Cell Lymphoma Network.Lancet. 2016 Aug 6;388(10044):565-75. doi: 10.1016/S0140-6736(16)00739-X. Epub 2016 Jun 14. Lancet. 2016. PMID: 27313086 Clinical Trial.
-
Mantle cell lymphoma international prognostic index but not pretransplantation induction regimen predicts survival for patients with mantle-cell lymphoma receiving high-dose therapy and autologous stem-cell transplantation.J Clin Oncol. 2011 Aug 1;29(22):3023-9. doi: 10.1200/JCO.2010.33.7055. Epub 2011 Jul 5. J Clin Oncol. 2011. PMID: 21730271 Free PMC article.
-
Immunotherapy with rituximab following high-dose therapy and autologous stem-cell transplantation for mantle cell lymphoma.Semin Oncol. 2002 Feb;29(1 Suppl 2):56-69. Semin Oncol. 2002. PMID: 11842390 Review.
-
Mantle cell lymphoma: therapeutic options in transplant-ineligible patients.Leuk Lymphoma. 2019 Nov;60(11):2622-2634. doi: 10.1080/10428194.2019.1605511. Epub 2019 Apr 25. Leuk Lymphoma. 2019. PMID: 31018735 Review.
Cited by
-
Real-world outcomes with ibrutinib in relapsed or refractory mantle cell lymphoma: a Danish population-based study.Blood Neoplasia. 2025 Jun 9;2(3):100128. doi: 10.1016/j.bneo.2025.100128. eCollection 2025 Aug. Blood Neoplasia. 2025. PMID: 40809191 Free PMC article.
-
Modified R-BAC plus BTK inhibitor regimen in newly diagnosed young patients with mantle cell lymphoma: a real-world retrospective study.Ann Hematol. 2024 Jun;103(6):2003-2012. doi: 10.1007/s00277-024-05648-5. Epub 2024 Feb 3. Ann Hematol. 2024. PMID: 38308020
-
Infections in patients with mantle cell lymphoma.Hemasphere. 2024 Jul 8;8(7):e121. doi: 10.1002/hem3.121. eCollection 2024 Jul. Hemasphere. 2024. PMID: 38978637 Free PMC article.
References
-
- Cheah CY, Opat S, Trotman J, Marlton P. Front-line management of indolent non-Hodgkin lymphoma in Australia. Part 2: mantle cell lymphoma and marginal zone lymphoma. Intern Med J. 2019;49(9):1070–1080. - PubMed
-
- Dreyling M, Geisler C, Hermine O, et al. Newly diagnosed and relapsed mantle cell lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2014;25(suppl 3):iii83–iii92. - PubMed
