

Association of baseline soluble immune checkpoints with the risk of relapse in PR3-ANCA vasculitis following induction of remission
- PMID: 35973802
- PMCID: PMC12341842
- DOI: 10.1136/ard-2022-222479
Association of baseline soluble immune checkpoints with the risk of relapse in PR3-ANCA vasculitis following induction of remission
Abstract
Objectives: We investigated whether soluble immune checkpoints (sICPs) predict treatment resistance, relapse and infections in patients with antineutrophil cytoplasm antibody (ANCA)-associated vasculitis (AAV).
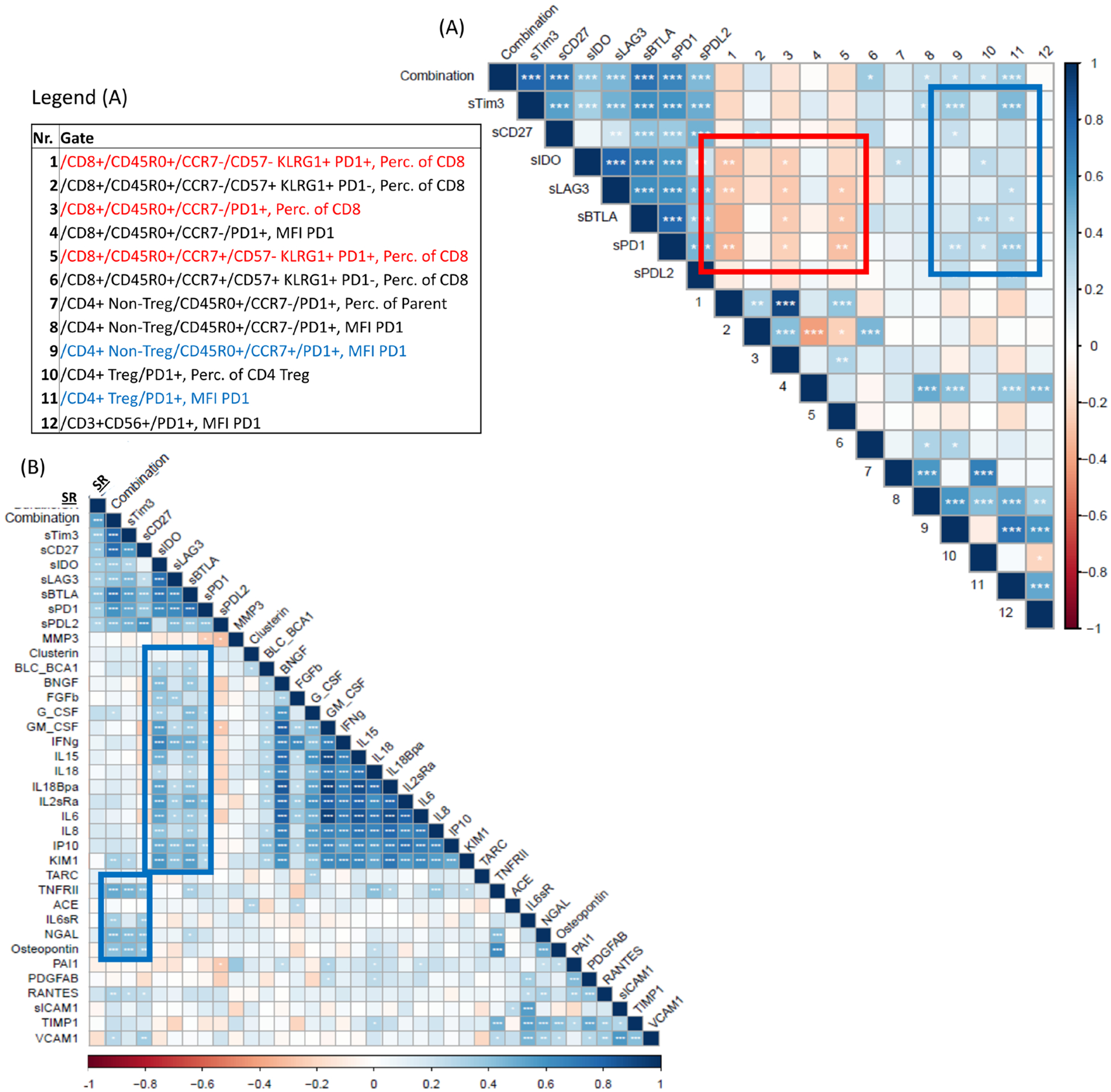
Methods: Plasma sICP concentrations from available samples obtained during conduct of the RAVE trial were measured by immunoabsorbent assays from patients with either proteinase 3 (PR3) or myeloperoxidase (MPO)-ANCA vasculitis and were correlated with clinical outcomes, a set of biomarkers and available flow cytometry analyses focusing on T cell subsets. Log-rank test was used to evaluate survival benefits, and optimal cut-off values of the marker molecules were calculated using Yeldons J.
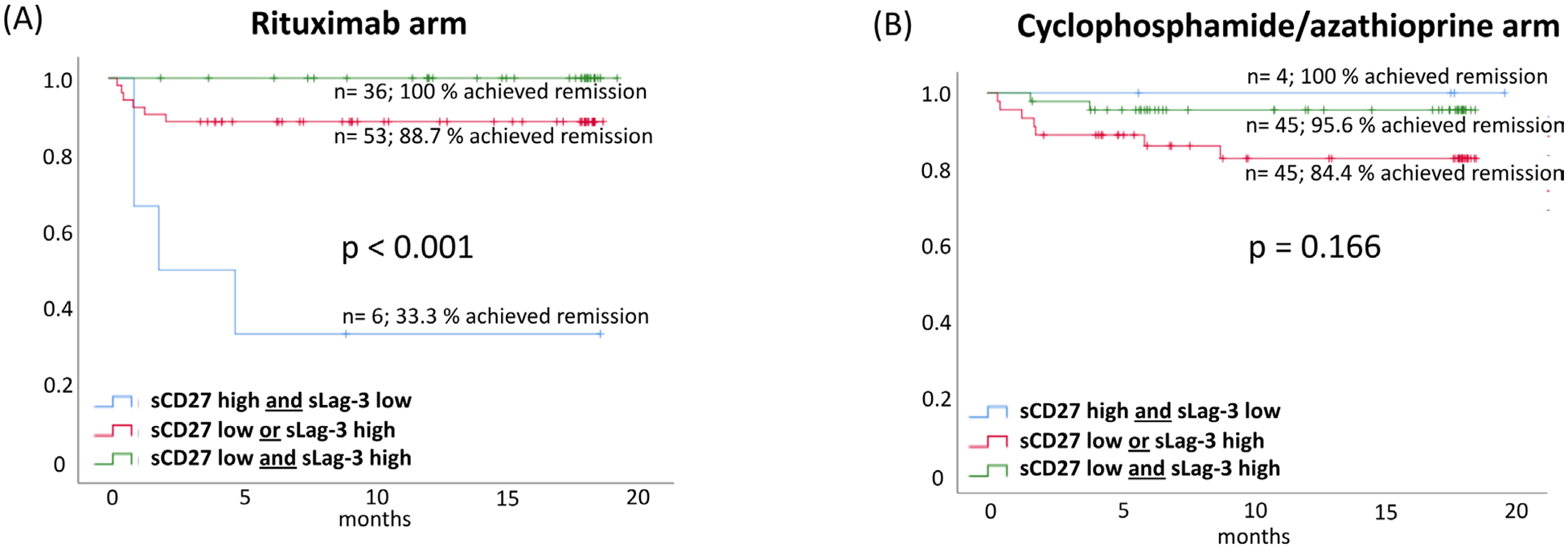
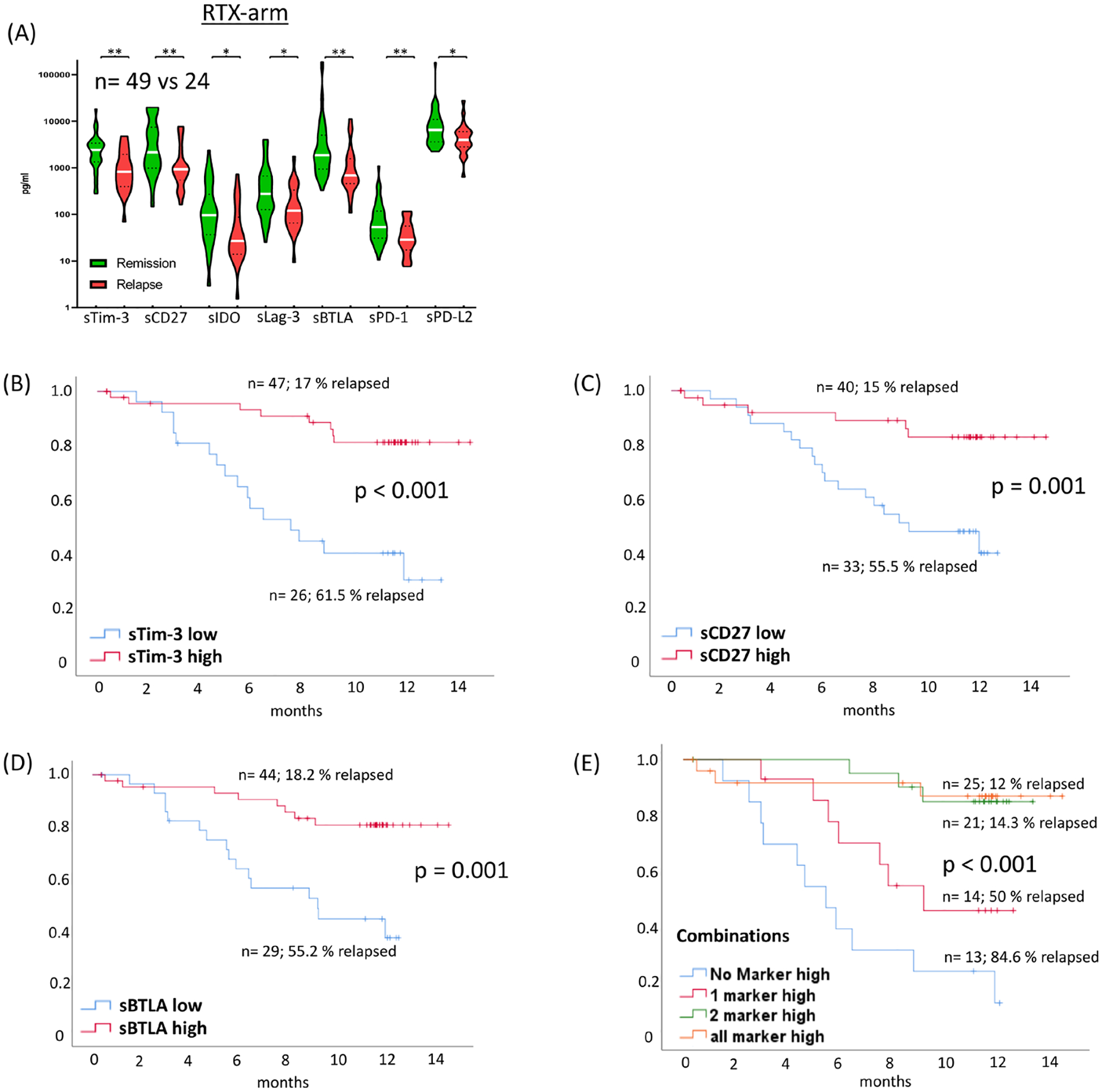
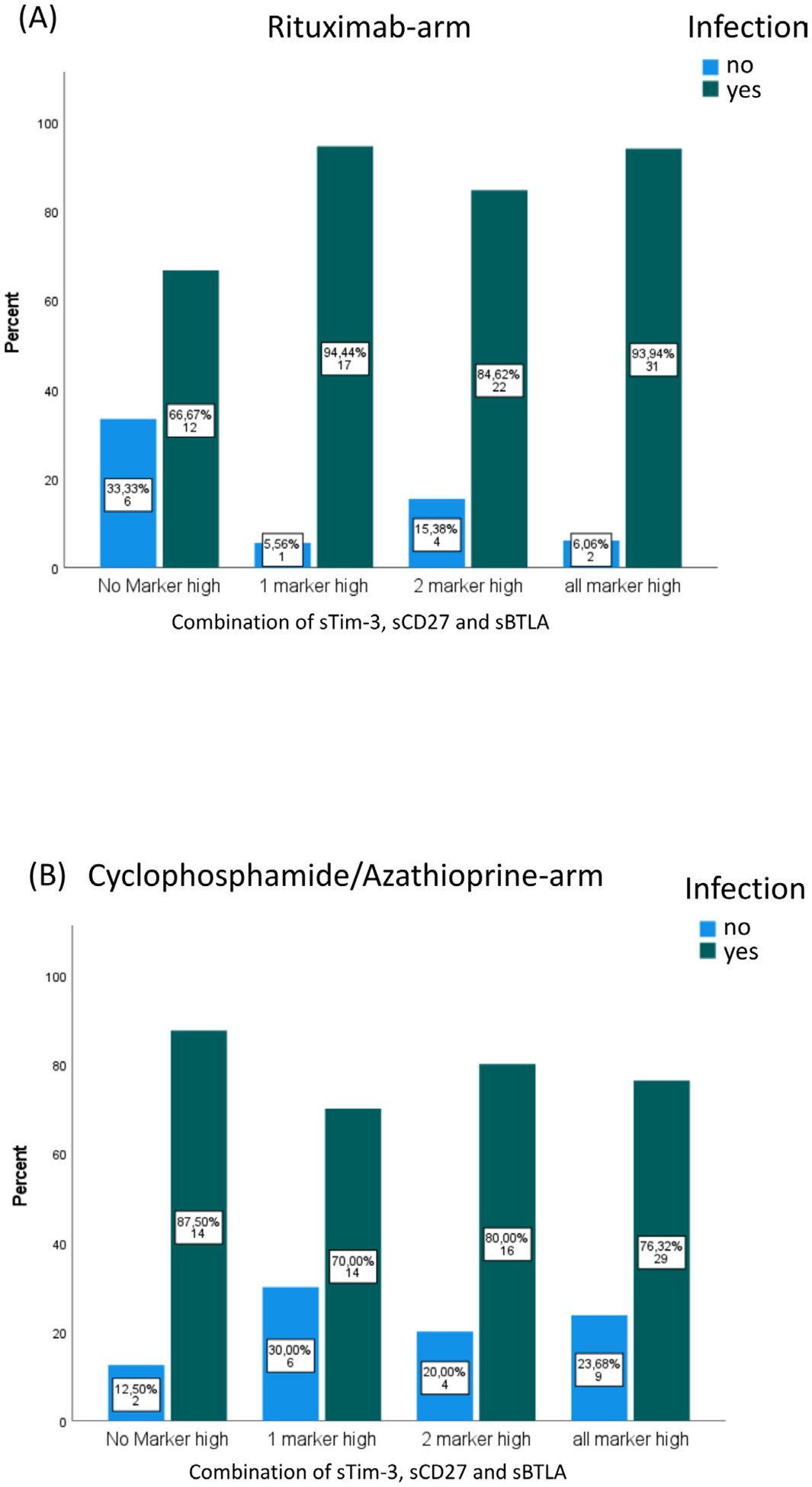
Results: Analysis of 189 plasma samples at baseline revealed higher concentrations of sTim-3, sCD27, sLag-3, sPD-1 and sPD-L2 in patients with MPO-ANCA vasculitis (n=62) as compared with PR3-ANCA vasculitis (n=127). Among patients receiving rituximab induction therapy (n=95), the combination of lower soluble (s)Lag-3 (<90 pg/mL) and higher sCD27 (>3000 pg/mL) predicted therapy failure. Twenty-four out of 73 patients (32.9%) in the rituximab arm reaching remission at 6 months relapsed during follow-up. In this subgroup, high baseline values of sTim-3 (>1200 pg/mL), sCD27 (>1250 pg/mL) and sBTLA (>1000 pg/mL) were associated with both sustained remission and infectious complications. These findings could not be replicated in 94 patients randomised to receive cyclophosphamide/azathioprine.
Conclusions: Patients with AAV treated with rituximab achieved remission less frequently when concentrations of sLag-3 were low and concentrations of sCD27 were high. Higher concentrations of sTim-3, sCD27 and sBTLA at baseline predicted relapse in patients treated with rituximab. These results require confirmation but may contribute to a personalised treatment approach of AAV.
Keywords: autoimmune diseases; rituximab; systemic vasculitis.
© Author(s) (or their employer(s)) 2023. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
