

A systems approach towards remote health-monitoring in older adults: Introducing a zero-interaction digital exhaust
- PMID: 35974156
- PMCID: PMC9381599
- DOI: 10.1038/s41746-022-00657-y
A systems approach towards remote health-monitoring in older adults: Introducing a zero-interaction digital exhaust
Abstract
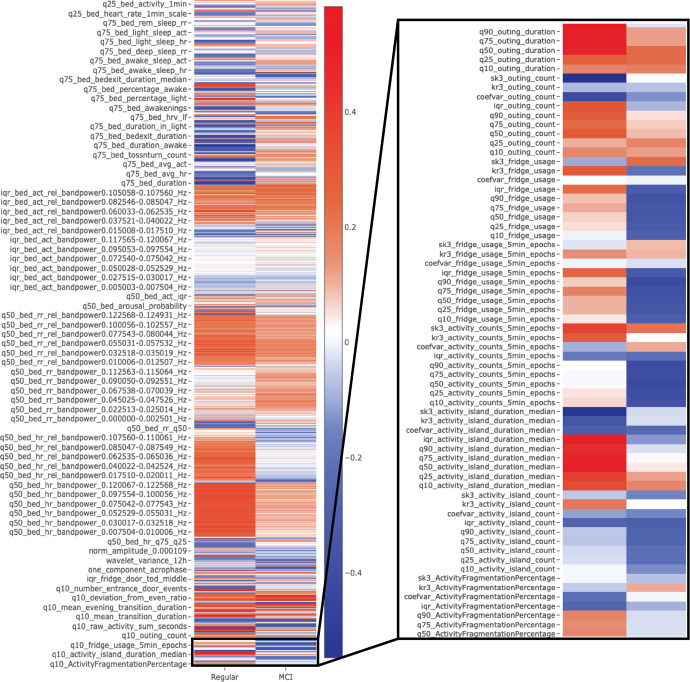
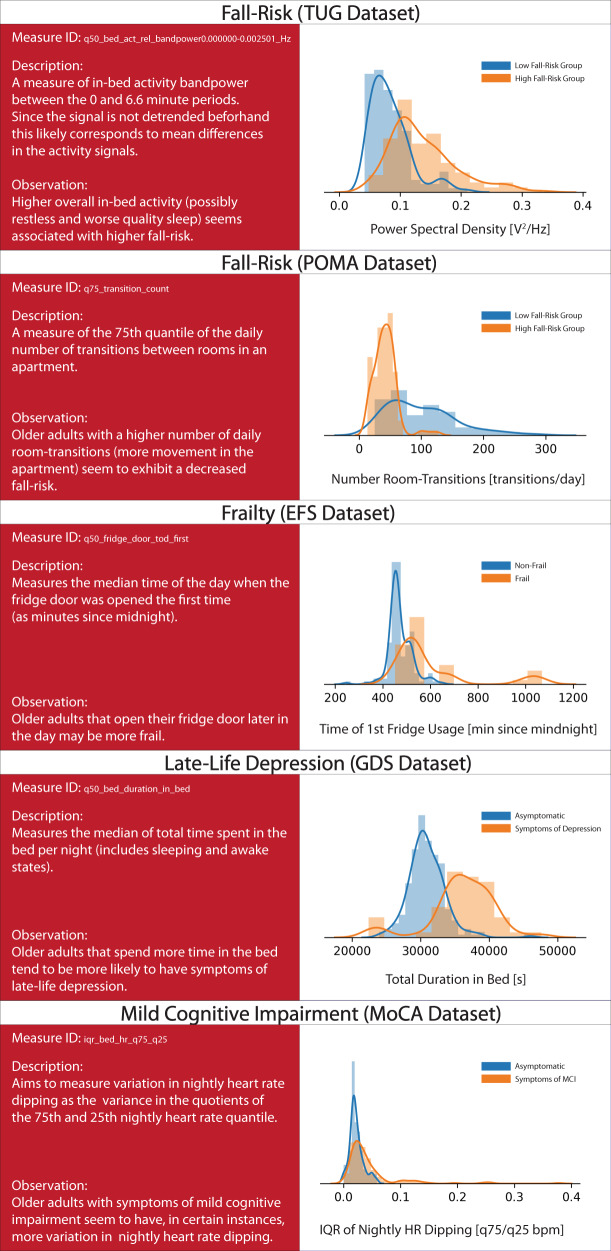
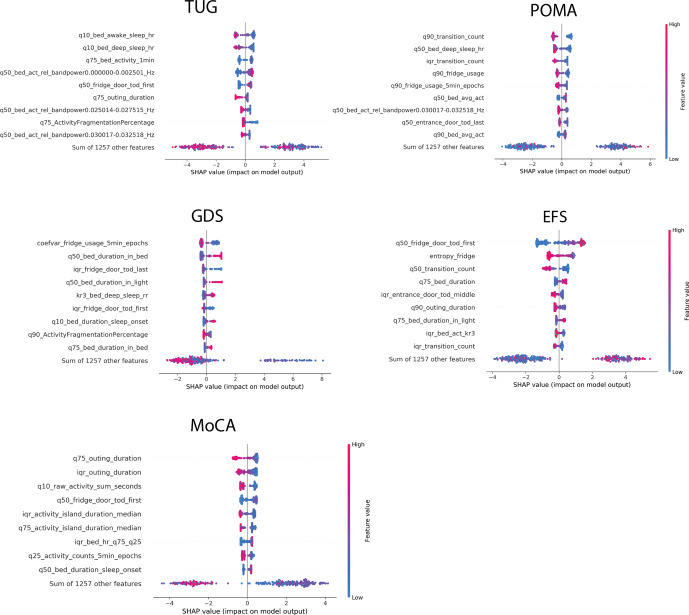
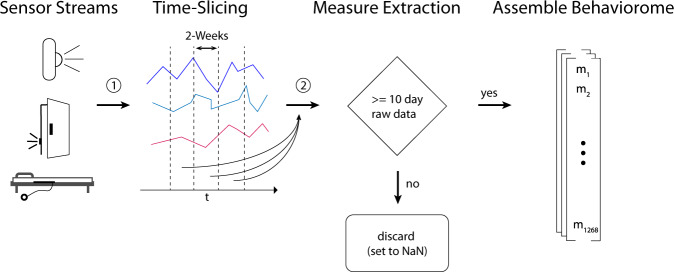
Using connected sensing devices to remotely monitor health is a promising way to help transition healthcare from a rather reactive to a more precision medicine oriented proactive approach, which could be particularly relevant in the face of rapid population ageing and the challenges it poses to healthcare systems. Sensor derived digital measures of health, such as digital biomarkers or digital clinical outcome assessments, may be used to monitor health status or the risk of adverse events like falls. Current research around such digital measures has largely focused on exploring the use of few individual measures obtained through mobile devices. However, especially for long-term applications in older adults, this choice of technology may not be ideal and could further add to the digital divide. Moreover, large-scale systems biology approaches, like genomics, have already proven beneficial in precision medicine, making it plausible that the same could also hold for remote-health monitoring. In this context, we introduce and describe a zero-interaction digital exhaust: a set of 1268 digital measures that cover large parts of a person's activity, behavior and physiology. Making this approach more inclusive of older adults, we base this set entirely on contactless, zero-interaction sensing technologies. Applying the resulting digital exhaust to real-world data, we then demonstrate the possibility to create multiple ageing relevant digital clinical outcome assessments. Paired with modern machine learning, we find these assessments to be surprisingly powerful and often on-par with mobile approaches. Lastly, we highlight the possibility to discover novel digital biomarkers based on this large-scale approach.
© 2022. The Author(s).
Conflict of interest statement
Dr. Philipp Buluschek and Dr. Narayan Schütz (effectively only after writing the article) were employed by DomoHealth SA, which is the manufacturer of one of the used sensor systems (PIR and door sensors). The remaining authors declare no competing financial or non-financial interests.
Figures
References
-
- Bloom DE, Canning D, Lubet A. Global population aging: Facts, challenges, solutions & perspectives. Daedalus. 2015;144:80–92. doi: 10.1162/DAED_a_00332. - DOI
