

Effects of ultrasound-guided alveolar recruitment manoeuvres compared with sustained inflation or no recruitment manoeuvres on atelectasis in laparoscopic gynaecological surgery as assessed by ultrasonography: a randomized clinical trial
- PMID: 35974310
- PMCID: PMC9380300
- DOI: 10.1186/s12871-022-01798-z
Effects of ultrasound-guided alveolar recruitment manoeuvres compared with sustained inflation or no recruitment manoeuvres on atelectasis in laparoscopic gynaecological surgery as assessed by ultrasonography: a randomized clinical trial
Abstract
Background: The majority of patients may experience atelectasis under general anesthesia, and the Trendelenburg position and pneumoperitoneum can aggravate atelectasis during laparoscopic surgery, which promotes postoperative pulmonary complications. Lung recruitment manoeuvres have been proven to reduce perioperative atelectasis, but it remains controversial which method is optimal. Ultrasonic imaging can be conducive to confirming the effect of lung recruitment manoeuvres. The purpose of our study was to assess the effects of ultrasound-guided alveolar recruitment manoeuvres by ultrasonography on reducing perioperative atelectasis and to check whether the effects of recruitment manoeuvres under ultrasound guidance (visual and semiquantitative) on atelectasis are superior to sustained inflation recruitment manoeuvres (classical and widely used) in laparoscopic gynaecological surgery.
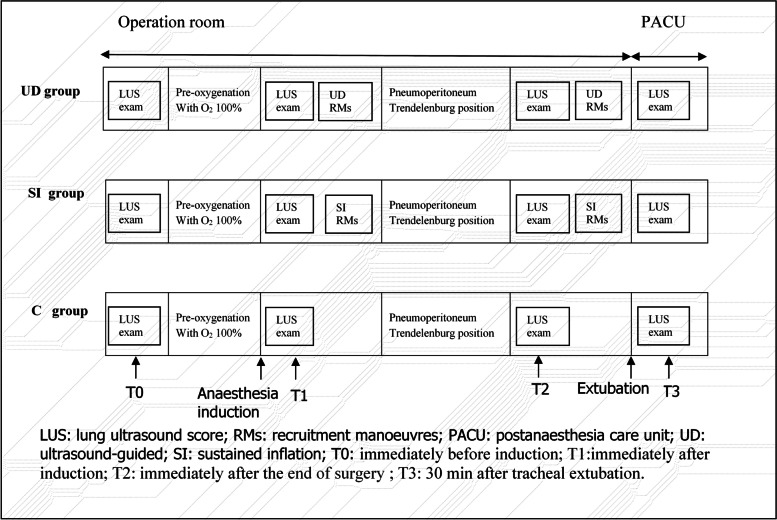
Methods: In this randomized, controlled, double-blinded study, women undergoing laparoscopic gynecological surgery were enrolled. Patients were randomly assigned to receive either lung ultrasound-guided alveolar recruitment manoeuvres (UD group), sustained inflation alveolar recruitment manoeuvres (SI group), or no RMs (C group) using a computer-generated table of random numbers. Lung ultrasonography was performed at four predefined time points. The primary outcome was the difference in lung ultrasound score (LUS) among groups at the end of surgery.
Results: Lung ultrasound scores in the UD group were significantly lower than those in both the SI group and the C group immediately after the end of surgery (7.67 ± 1.15 versus 9.70 ± 102, difference, -2.03 [95% confidence interval, -2.77 to -1.29], P < 0.001; 7.67 ± 1.15 versus 11.73 ± 1.96, difference, -4.07 [95% confidence interval, -4.81 to -3.33], P < 0.001;, respectively). The intergroup differences were sustained until 30 min after tracheal extubation (9.33 ± 0.96 versus 11.13 ± 0.97, difference, -1.80 [95% confidence interval, -2.42 to -1.18], P < 0.001; 9.33 ± 0.96 versus 10.77 ± 1.57, difference, -1.43 [95% confidence interval, -2.05 to -0.82], P < 0.001;, respectively). The SI group had a significantly lower LUS than the C group at the end of surgery (9.70 ± 1.02 versus 11.73 ± 1.96, difference, -2.03 [95% confidence interval, -2.77 to -1.29] P < 0.001), but the benefit did not persist 30 min after tracheal extubation.
Conclusions: During general anesthesia, ultrasound-guided recruitment manoeuvres can reduce perioperative aeration loss and improve oxygenation. Furthermore, these effects of ultrasound-guided recruitment manoeuvres on atelectasis are superior to sustained inflation recruitment manoeuvres.
Trial registration: Chictr.org.cn, ChiCTR2100042731, Registered 27 January 2021, www.chictr.org.cn .
Keywords: Atelectasis; General anesthesia; Recruitment manoeuvres; Sustained inflation; Ultrasound-guided.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures




Similar articles
-
Ultrasound-guided versus conventional lung recruitment manoeuvres in laparoscopic gynaecological surgery: A randomised controlled trial.Eur J Anaesthesiol. 2021 Mar 1;38(3):275-284. doi: 10.1097/EJA.0000000000001435. Eur J Anaesthesiol. 2021. PMID: 33399385 Clinical Trial.
-
Effects of positive end-expiratory pressure/recruitment manoeuvres compared with zero end-expiratory pressure on atelectasis during open gynaecological surgery as assessed by ultrasonography: a randomised controlled trial.Br J Anaesth. 2020 Jan;124(1):101-109. doi: 10.1016/j.bja.2019.09.040. Epub 2019 Nov 14. Br J Anaesth. 2020. PMID: 31733807 Clinical Trial.
-
Ultrasound-guided versus conventional lung recruitment manoeuvres in thoracic surgery: a randomised controlled study.J Clin Monit Comput. 2024 Jun;38(3):731-739. doi: 10.1007/s10877-024-01134-5. Epub 2024 Feb 17. J Clin Monit Comput. 2024. PMID: 38368302 Clinical Trial.
-
Anesthesia considerations to reduce motion and atelectasis during advanced guided bronchoscopy.BMC Pulm Med. 2021 Jul 17;21(1):240. doi: 10.1186/s12890-021-01584-6. BMC Pulm Med. 2021. PMID: 34273966 Free PMC article.
-
The role of lung ultrasound for detecting atelectasis, consolidation, and/or pneumonia in the adult cardiac surgery population: A scoping review of the literature.Aust Crit Care. 2024 Jan;37(1):193-201. doi: 10.1016/j.aucc.2023.08.002. Epub 2023 Sep 13. Aust Crit Care. 2024. PMID: 37709655
Cited by
-
Setting positive end-expiratory pressure: lung and diaphragm ultrasound.Curr Opin Crit Care. 2024 Feb 1;30(1):53-60. doi: 10.1097/MCC.0000000000001119. Epub 2023 Nov 17. Curr Opin Crit Care. 2024. PMID: 38085883 Free PMC article. Review.
-
Effect of driving pressure-guided individualized positive end-expiratory pressure (PEEP) ventilation strategy on postoperative atelectasis in patients undergoing laparoscopic surgery as assessed by ultrasonography: study protocol for a prospective randomized controlled trial.Trials. 2025 Mar 26;26(1):106. doi: 10.1186/s13063-025-08819-5. Trials. 2025. PMID: 40140868 Free PMC article.
-
Effects of ultrasound-guided recruitment manoeuvres on postoperative pulmonary complications in laparoscopic bariatric surgery patients: study protocol for a randomised clinical trial.Trials. 2025 Jan 9;26(1):13. doi: 10.1186/s13063-024-08702-9. Trials. 2025. PMID: 39789661 Free PMC article.
-
Intra-operative ventilation strategies and their impact on clinical outcomes: a systematic review and network meta-analysis of randomised trials.Anaesthesia. 2025 Aug;80(8):973-987. doi: 10.1111/anae.16600. Epub 2025 Mar 25. Anaesthesia. 2025. PMID: 40133080 Free PMC article.
-
An anesthesia-centered bundle to reduce postoperative pulmonary complications: The PRIME-AIR study protocol.PLoS One. 2023 Apr 6;18(4):e0283748. doi: 10.1371/journal.pone.0283748. eCollection 2023. PLoS One. 2023. PMID: 37023031 Free PMC article.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
