

Association Between Red Blood Cell Distribution Width-Albumin Ratio and Hospital Mortality in Chronic Obstructive Pulmonary Disease Patients Admitted to the Intensive Care Unit: A Retrospective Study
- PMID: 35975033
- PMCID: PMC9376003
- DOI: 10.2147/COPD.S371765
Association Between Red Blood Cell Distribution Width-Albumin Ratio and Hospital Mortality in Chronic Obstructive Pulmonary Disease Patients Admitted to the Intensive Care Unit: A Retrospective Study
Abstract
Purpose: High levels of red blood cell distribution width (RDW) and hypoalbuminemia are markers of poor prognosis in chronic obstructive pulmonary disease (COPD) patients. However, few studies have shown that the red blood cell distribution width-albumin ratio (RAR) is related to the mortality of COPD. This study aimed to explore the relationship between RAR and hospital mortality in COPD patients admitted to the intensive care unit (ICU).
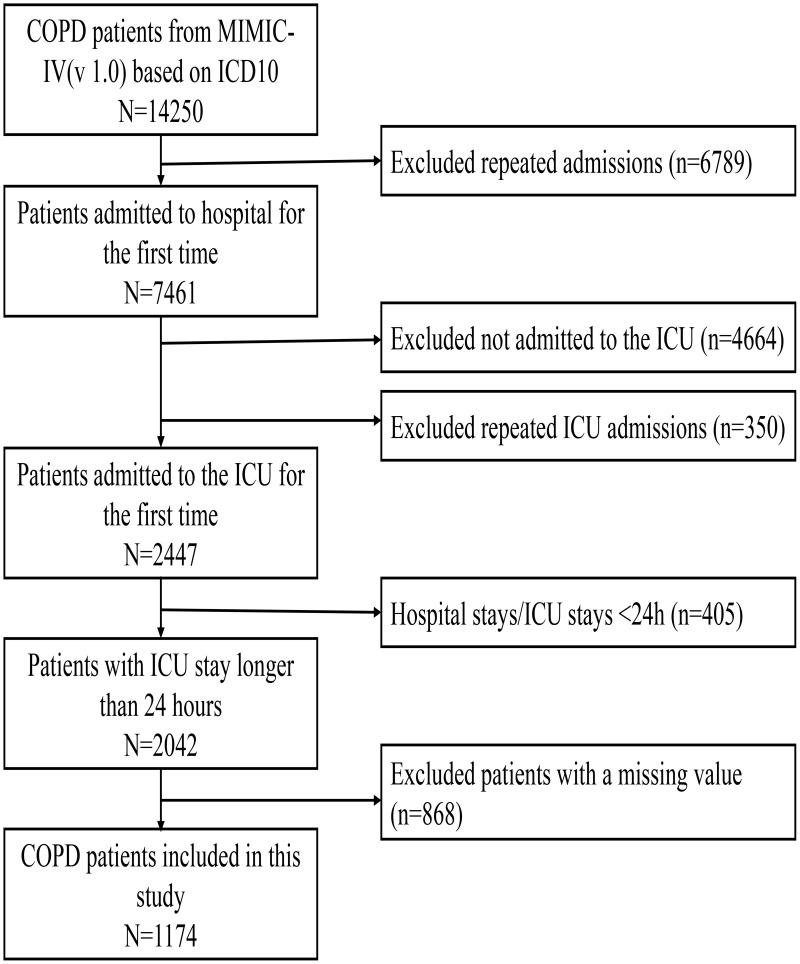
Patients and methods: Patients were retrospectively incorporated from the Medical Information Mart for Intensive Care IV (MIMIC-IV) database and divided into two groups by a cutoff value of RAR. Propensity score matching (PSM) was performed to adjust for the imbalance of covariates. Logistic regression models and subgroup analyses were carried out to investigate the relationship between RAR and hospital mortality. The receiver operating characteristic (ROC) curve was used to evaluate the predictive performance of RAR and decision curve analysis (DCA) to assess the clinical utility.
Results: In total, 1174 patients were finally identified from the MIMIC-IV database. The cutoff value for RAR was 5.315%/g/dL. After PSM at a 1:1 ratio, 638 patients were included in the matched cohort. In the original and matched cohorts, the high RAR group had higher hospital mortality and longer hospital stays. Logistic regression analysis suggested that RAR was an independent risk factor for hospital mortality. The areas under the ROC curve in the original and matched cohorts were 0.706 and 0.611, respectively, which were larger than applying RDW alone (the original cohort: 0.600, the matched cohort: 0.514). The DCA indicated that RAR had a clinical utility.
Conclusion: A higher RAR (>5.315%/g/dL) was associated with hospital mortality in COPD patients admitted to ICU. As an easily available peripheral blood marker, RAR can predict hospital mortality in critically ill patients with COPD independently.
Keywords: MIMIC-IV; albumin; chronic obstructive pulmonary disease; hospital mortality; red blood cell distribution width.
© 2022 Qiu et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures




References
-
- Wang H, Naghavi M, Allen C, et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: a systematic analysis for the global burden of disease study 2015. Lancet. 2016;388(10053):1459–1544. doi: 10.1016/S0140-6736(16)31012-1 - DOI - PMC - PubMed
-
- Afessa B, Morales IJ, Scanlon PD, Peters SG. Prognostic factors, clinical course, and hospital outcome of patients with chronic obstructive pulmonary disease admitted to an intensive care unit for acute respiratory failure. Crit Care Med. 2002;30(7):1610–1615. doi: 10.1097/00003246-200207000-00035 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
