

Healthcare Utilization and Costs Among US Adolescents With Alopecia Areata
- PMID: 35975139
- PMCID: PMC9338344
- DOI: 10.36469/001c.36229
Healthcare Utilization and Costs Among US Adolescents With Alopecia Areata
Abstract
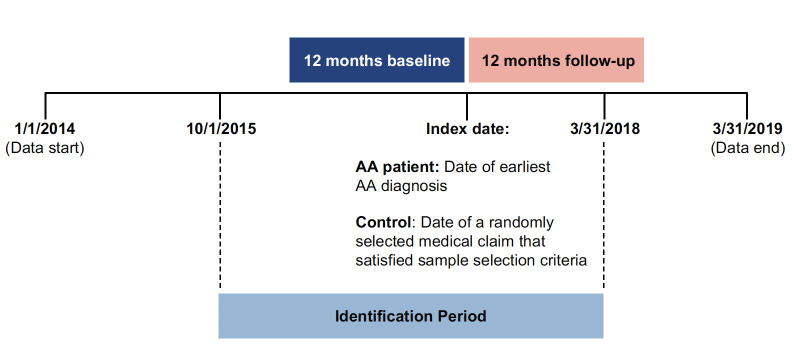
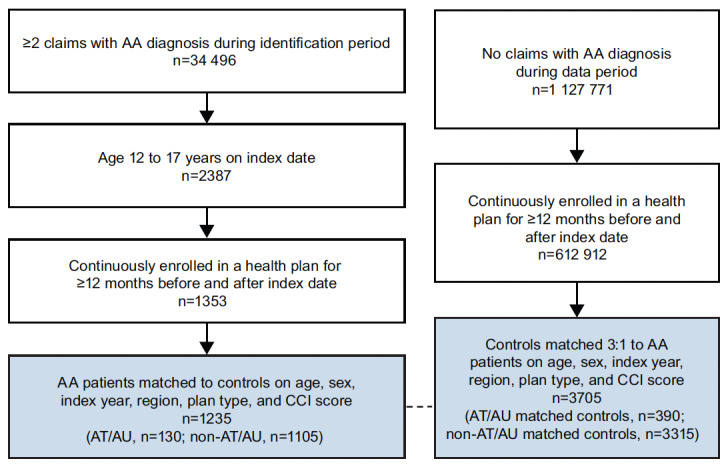
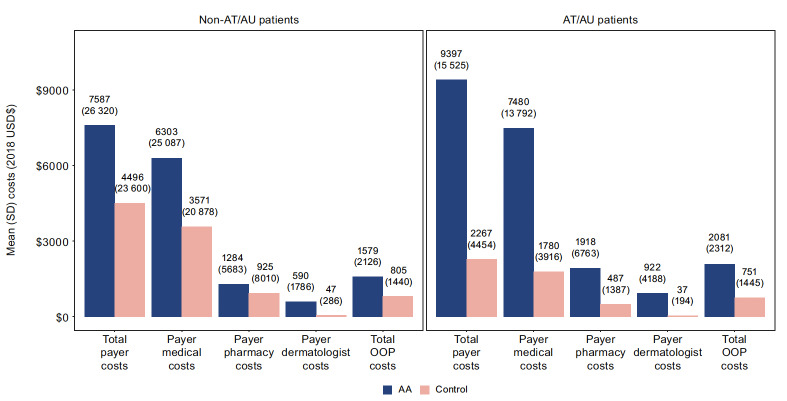
Background: Alopecia areata (AA) is an autoimmune disease of hair loss affecting people of all ages. Alopecia totalis (AT) and universalis (AU) involve scalp and total body hair loss, respectively. AA significantly affects quality of life, but evidence on the economic burden in adolescents is limited. Objectives: To assess healthcare resource utilization (HCRU) and all-cause direct healthcare costs, including out-of-pocket (OOP) costs, of US adolescents with AA. Methods: IBM MarketScan® Commercial and Medicare databases were used to identify patients aged 12-17 years with ≥2 claims with AA/AT/AU diagnosis (prevalent cases), from October 1, 2015, to March 31, 2018, enrolled for ≥12 months before and after the first AA diagnosis (index). Patients were matched 1:3 to non-AA controls on index year, demographics, plan type, and Charlson Comorbidity Index. Per patient per year HCRU and costs were compared post-index. Results: Patients comprised 130 AT/AU adolescents and 1105 non-AT/AU adolescents (53.8% female; mean age, 14.6 years). Post-index, AT/AU vs controls had more outpatient (14.5 vs 7.1) and dermatologist (3.6 vs 0.3) visits, higher mean plan costs ($9397 vs $2267), including medical ($7480 vs $1780) and pharmacy ($1918 vs $487) costs, and higher OOP costs ($2081 vs $751) (all P<.001). The non-AT/AU cohort vs controls had more outpatient (11.6 vs 8.0) and dermatologist (3.4 vs 0.4) visits, higher mean plan costs ($7587 vs $4496), and higher OOP costs ($1579 vs $805) (all P<.001). Discussion: This large-sample, real-world analysis found that adolescents with prevalent AA had significantly higher HCRU and all-cause costs than matched controls. The greater burden was driven by more frequent outpatient visits, and higher payer medical and pharmacy costs in comparison with controls. Oral corticosteroid use was higher among patients with AT/AU; topical and injectable corticosteroid use was higher for non-AT/AU. Although the data preclude the identification of AA-attributable costs, the matched-control design allows an estimation of incremental all-cause costs associated with AA. Conclusions: Adolescents with AA incurred substantial incremental healthcare costs, with greater costs incurred among those with AT/AU. Study findings suggest that AA incurs costs as a medical condition with a high burden on adolescent patients and health plans.
Keywords: adolescents; alopecia areata; corticosteroids; healthcare costs; retrospective claims study.
Conflict of interest statement
M.R., K.G., and V.S. were employees of Pfizer and held stocks/stock options of Pfizer at the time of study conduct and analyses. E.S., C.C., T.W., N.D., and J.S. are employees of Analysis Group, Inc, a consultancy that received payment from Pfizer for participation in this analysis. A.M. reports consulting fees from AbbVie, Bioniz, Digital Diagnostics, Eli Lilly, hims™, and Pfizer; has received licensing/royalties from Concert and Pfizer; has served on the medical advisory board for hims™; has been an investigator in clinical trials for Concert and Eli Lilly; and is an associate editor of JAMA Dermatology.
Figures
Similar articles
-
All-cause health care resource utilization and costs among adults with alopecia areata: A retrospective claims database study in the United States.J Manag Care Spec Pharm. 2022 Apr;28(4):426-434. doi: 10.18553/jmcp.2022.28.4.426. J Manag Care Spec Pharm. 2022. PMID: 35332790 Free PMC article.
-
Trends in Prevalence and Incidence of Alopecia Areata, Alopecia Totalis, and Alopecia Universalis Among Adults and Children in a US Employer-Sponsored Insured Population.JAMA Dermatol. 2023 Apr 1;159(4):411-418. doi: 10.1001/jamadermatol.2023.0002. JAMA Dermatol. 2023. PMID: 36857069 Free PMC article.
-
Comparing the burden of illness in patients with alopecia areata vs atopic dermatitis in the US population from a payer perspective.J Manag Care Spec Pharm. 2023 Apr;29(4):409-419. doi: 10.18553/jmcp.2023.29.4.409. J Manag Care Spec Pharm. 2023. PMID: 36989453 Free PMC article.
-
Childhood Alopecia Areata: An Overview of Treatment and Recent Patents.Recent Pat Inflamm Allergy Drug Discov. 2020;14(2):117-132. doi: 10.2174/1872213X14999200728145822. Recent Pat Inflamm Allergy Drug Discov. 2020. PMID: 32723274 Review.
-
Healthcare Resource Utilization (HCRU) and Direct Medical Costs Associated with Long COVID or Post-COVID-19 Conditions: Findings from a Literature Review.J Mark Access Health Policy. 2025 Feb 12;13(1):7. doi: 10.3390/jmahp13010007. eCollection 2025 Mar. J Mark Access Health Policy. 2025. PMID: 39990183 Free PMC article. Review.
Cited by
-
Overview of alopecia areata for managed care and payer stakeholders in the United States.J Manag Care Spec Pharm. 2023 Jul;29(7):848-856. doi: 10.18553/jmcp.2023.22371. Epub 2023 May 23. J Manag Care Spec Pharm. 2023. PMID: 37219075 Free PMC article.
-
Efficacy and safety of compound glycyrrhizin in patients with alopecia areata: a systematic review and meta-analysis.Ann Med. 2025 Dec;57(1):2491659. doi: 10.1080/07853890.2025.2491659. Epub 2025 Apr 23. Ann Med. 2025. PMID: 40265259 Free PMC article.
-
Incidence Rates of Infections, Malignancies, Thromboembolism, and Cardiovascular Events in an Alopecia Areata Cohort from a US Claims Database.Dermatol Ther (Heidelb). 2023 Aug;13(8):1733-1746. doi: 10.1007/s13555-023-00937-9. Epub 2023 Jun 10. Dermatol Ther (Heidelb). 2023. PMID: 37296372 Free PMC article.
-
A retrospective analysis of disease epidemiology, comorbidities, treatment patterns, and healthcare resource utilization of alopecia areata in the United Arab Emirates using claims database.J Dermatol. 2024 Sep;51(9):1157-1171. doi: 10.1111/1346-8138.17381. Epub 2024 Jul 25. J Dermatol. 2024. PMID: 39051178 Free PMC article.
-
Editorial: Advances in evaluation and management of hair loss disorders.Front Med (Lausanne). 2023 Jan 20;10:1131286. doi: 10.3389/fmed.2023.1131286. eCollection 2023. Front Med (Lausanne). 2023. PMID: 36744146 Free PMC article. No abstract available.
References
-
- Alopecia areata: disease characteristics, clinical evaluation, and new perspectives on pathogenesis. Strazzulla Lauren C., Wang Eddy Hsi Chun, Avila Lorena, Lo Sicco Kristen, Brinster Nooshin, Christiano Angela M., Shapiro Jerry. Jan;2018 Journal of the American Academy of Dermatology. 78(1):1–12. doi: 10.1016/j.jaad.2017.04.1141. doi: 10.1016/j.jaad.2017.04.1141. - DOI - DOI - PubMed
-
- Alopecia areata update: part I. Clinical picture, histopathology, and pathogenesis. Alkhalifah Abdullah, Alsantali Adel, Wang Eddy, McElwee Kevin J., Shapiro Jerry. Feb;2010 Journal of the American Academy of Dermatology. 62(2):177–188. doi: 10.1016/j.jaad.2009.10.032. doi: 10.1016/j.jaad.2009.10.032. - DOI - DOI - PubMed
LinkOut - more resources
Full Text Sources