

Freehand S2-Alar-Iliac Screw Placement Technique in Lumbosacral Spinal Tumors: A Preliminary Study
- PMID: 35975359
- PMCID: PMC9483049
- DOI: 10.1111/os.13434
Freehand S2-Alar-Iliac Screw Placement Technique in Lumbosacral Spinal Tumors: A Preliminary Study
Abstract
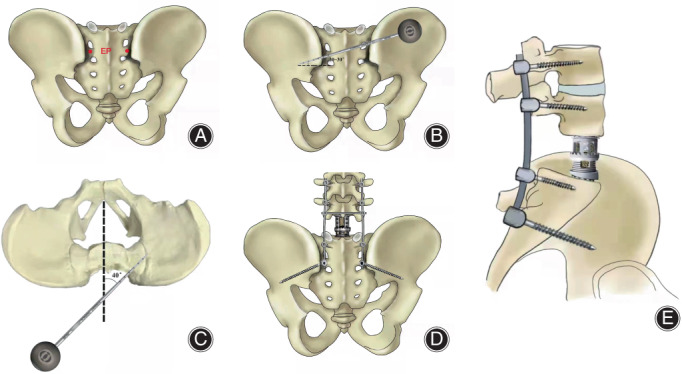
Objective: S2-alar-iliac (S2AI) screw technique is widely used in spinal surgery, but it is rarely seen in the field of spinal tumors. The aim of the study is to report the preliminary outcomes of the freehand S2AI screw fixation after lumbosaral tumor resection.
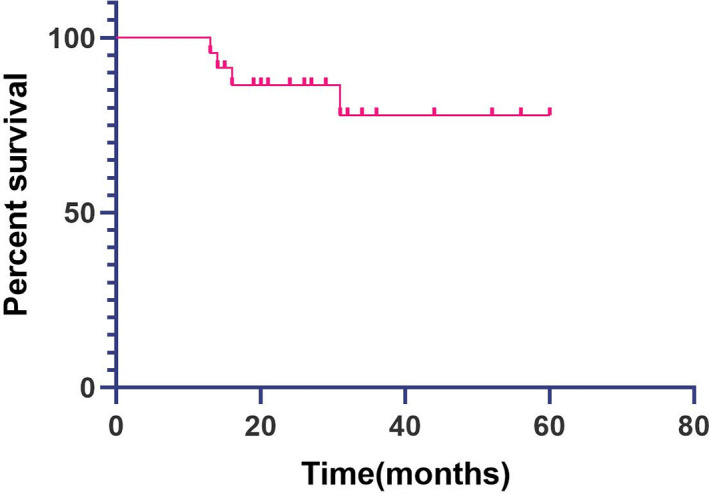
Methods: The records of patients with lumbosacral tumor who underwent S2AI screw fixation between November 2016 to November 2020 at our center were reviewed retrospectively. Outcome measures included operative time, blood loss, complications, accuracy of screws, screw breach, and overall survival. Mean ± standard deviation or range was used to present continuous variables. Kaplan-Meier curve was used to present postoperative survival.
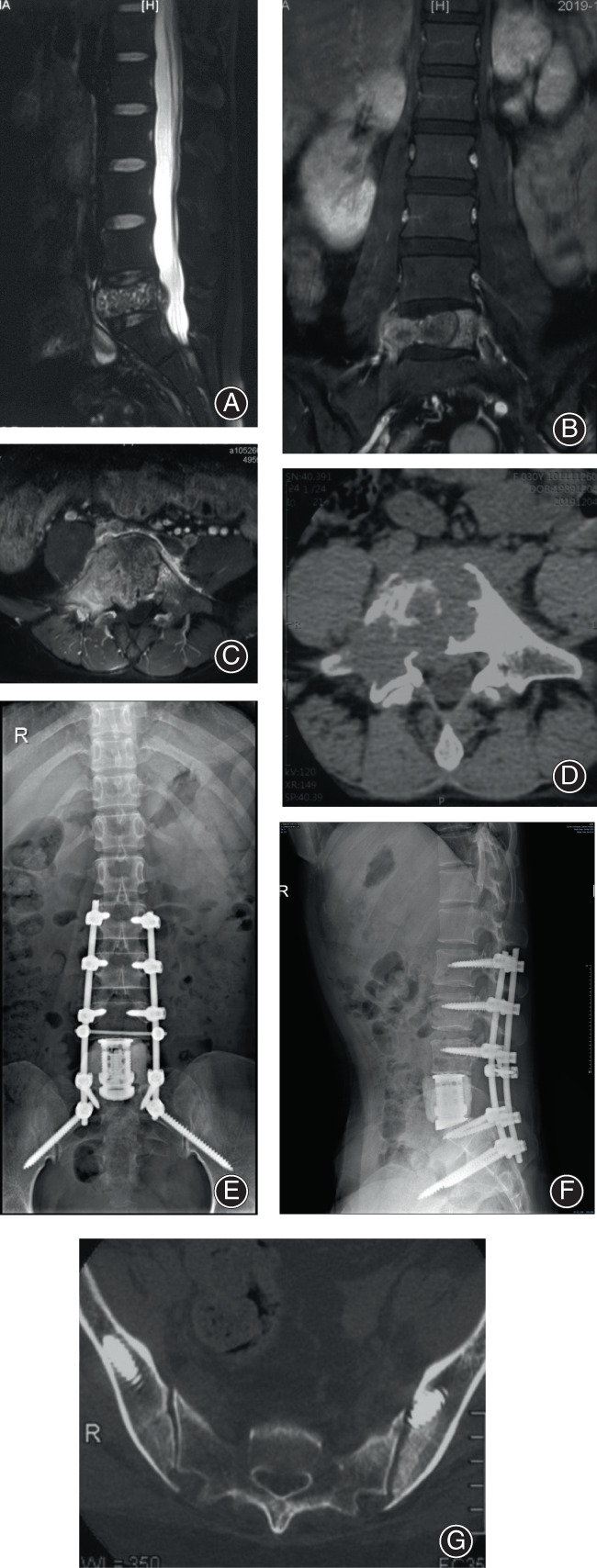
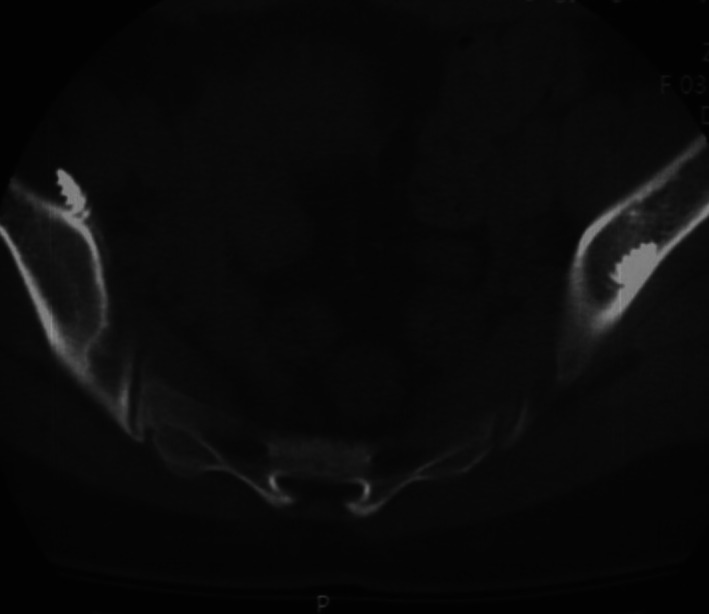
Results: A total of 23 patients were identified in this study, including 12 males and 11 females, with an average age of 47.3 ± 14.5 (range,15-73). The mean operation time was 224.6 ± 54.1 (range, 155-370 min). The average estimated blood loss was 1560.9 ± 887.0 (600-4000 ml). A total of 46 S2AI screws were implanted by freehand technique. CT scans showed three (6.5%) screws had penetrated the iliac cortex, indicating 93.5% implantation accuracy rate. No complications of iatrogenic neurovascular or visceral structure were observed. The average follow-up time was 31.6 ± 15.3 months (range, 13-60 months). Two patients' postoperative plain radiography showed lucent zone around the screw. One patient underwent reoperation for wound delayed infection. At the latest follow-up, eight patients had tumor-free survival, 11 had survival with tumor, and four died of disease.
Conclusion: The freehand S2AI screw technique is reproducible, safe, and reliable in the management of lumbosacral spinal tumors.
Keywords: S2-alar-iliac screw; freehand; lumbosacral fixation; lumbosacral spine; tumor.
© 2022 The Authors. Orthopaedic Surgery published by Tianjin Hospital and John Wiley & Sons Australia, Ltd.
Conflict of interest statement
There were no conflicts of interest in this study.
Figures
References
-
- Kebaish KM. Sacropelvic fixation: techniques and complications. Spine. 2010;35:2245–51. - PubMed
-
- Lombardi JM, Shillingford JN, Lenke LG, Lehman RA. Sacropelvic fixation: when, why, how? Neurosurg Clin N Am. 2018;29:389–97. - PubMed
-
- Moshirfar A, Rand FF, Sponseller PD, et al. Pelvic fixation in spine surgery. Historical overview, indications, biomechanical relevance, and current techniques. J Bone Joint Surg Am. 2005;87:89–106. - PubMed
-
- Jain A, Hassanzadeh H, Strike SA, Menga EN, Sponseller PD, Kebaish KM. Pelvic fixation in adult and pediatric spine surgery: historical perspective, indications, and techniques. J Bone Joint Surg Am. 2015;97:1521–8. - PubMed
-
- Sponseller PD. The S2 portal to the ilium. Semin Spine Surg. 2007;2:83–7.
MeSH terms
LinkOut - more resources
Full Text Sources
