

Effect of GBCA Use on Detection and Diagnostic Performance of the Central Vein Sign: Evaluation Using a 3-T FLAIR* Sequence in Patients With Suspected Multiple Sclerosis
- PMID: 35975888
- PMCID: PMC10016223
- DOI: 10.2214/AJR.22.27731
Effect of GBCA Use on Detection and Diagnostic Performance of the Central Vein Sign: Evaluation Using a 3-T FLAIR* Sequence in Patients With Suspected Multiple Sclerosis
Abstract
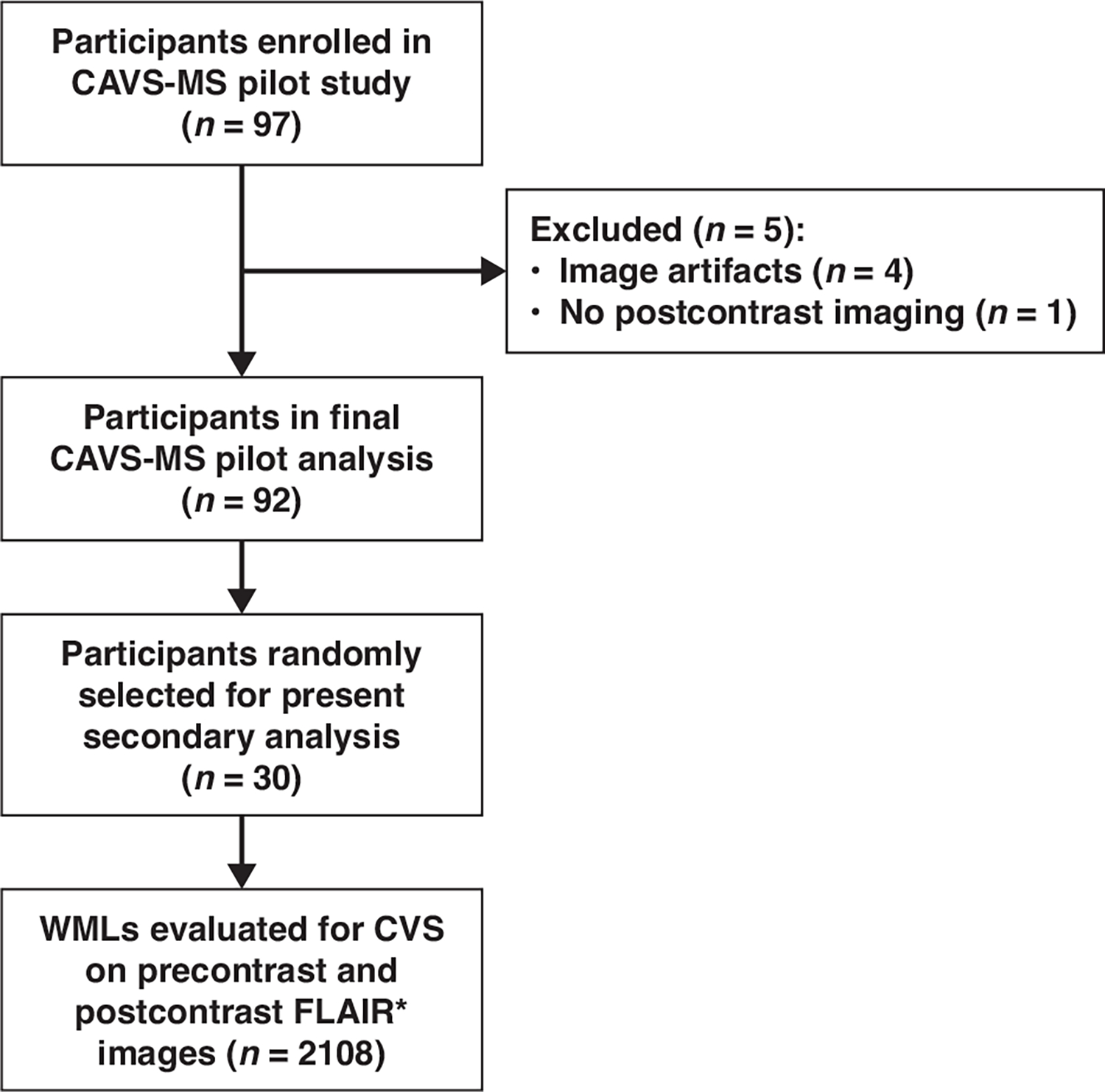
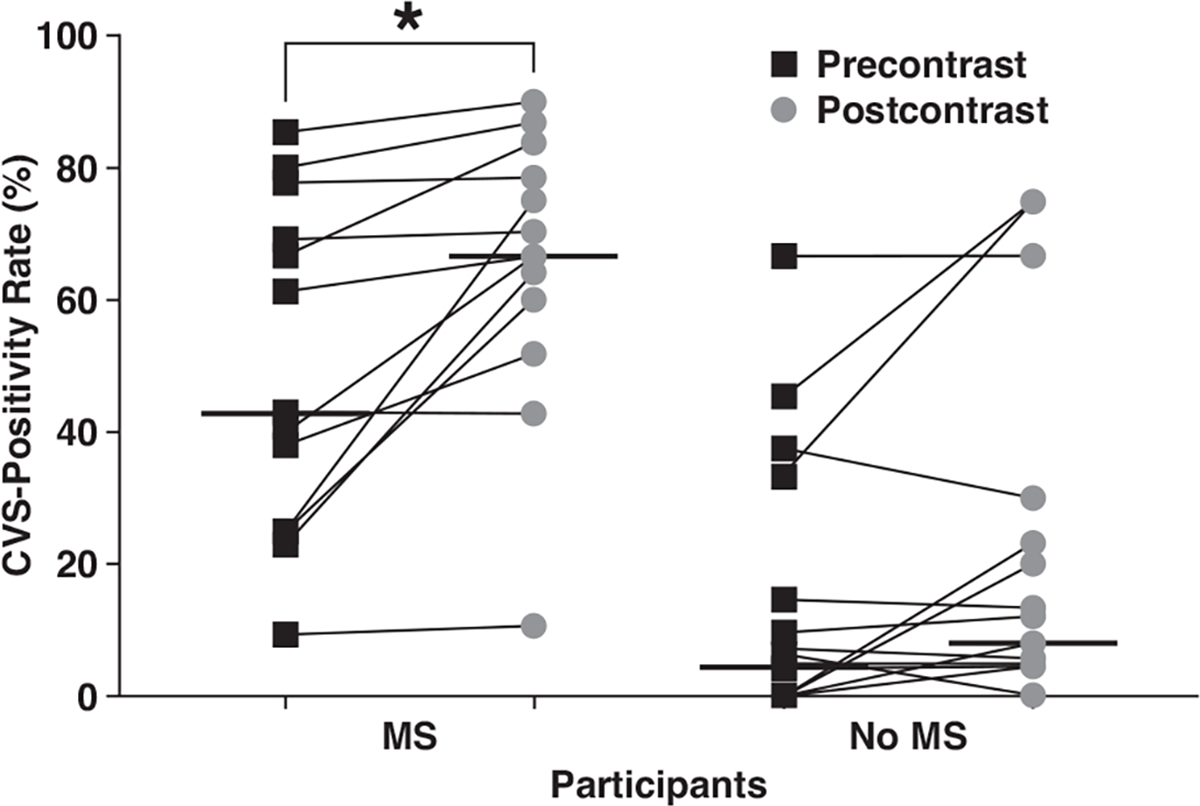
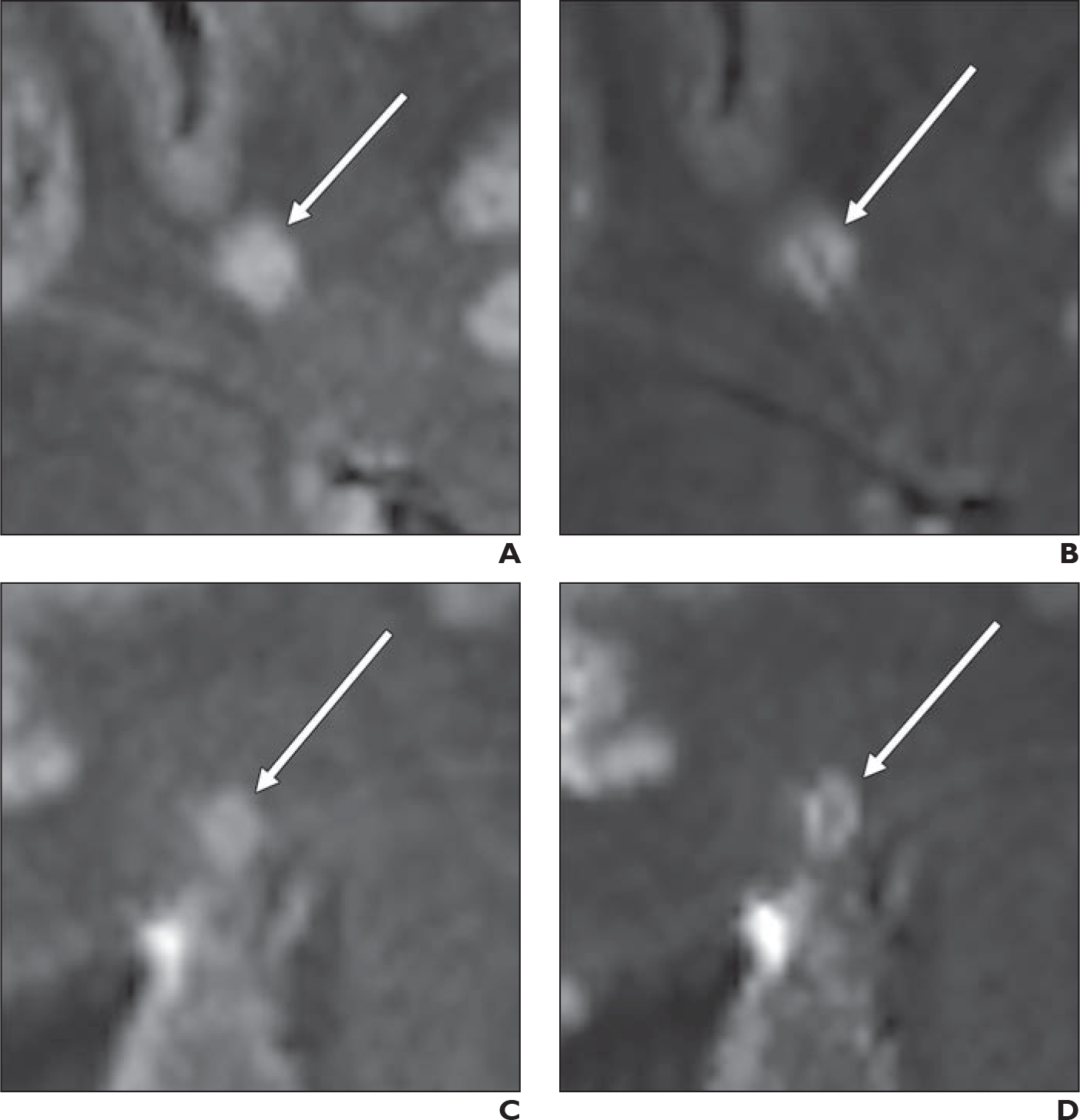
BACKGROUND. The central vein sign (CVS) is a proposed MRI biomarker of multiple sclerosis (MS). The impact of gadolinium-based contrast agent (GBCA) administration on CVS evaluation remains poorly investigated. OBJECTIVE. The purpose of this study was to assess the effect of GBCA use on CVS detection and on the diagnostic performance of the CVS for MS using a 3-T FLAIR* sequence. METHODS. This study was a secondary analysis of data from the pilot study for the prospective multicenter Central Vein Sign: A Diagnostic Biomarker in Multiple Sclerosis (CAVS-MS), which recruited adults with suspected MS from April 2018 to February 2020. Participants underwent 3-T brain MRI including FLAIR and precontrast and post-contrast echo-planar imaging T2*-weighted acquisitions. Postprocessing was used to generate combined FLAIR and T2*-weighted images (hereafter, FLAIR*). MS diagnoses were established using the 2017 McDonald criteria. Thirty participants (23 women, seven men; mean age, 45 years) were randomly selected from the CAVS-MS pilot study cohort. White matter lesions (WMLs) were marked using FLAIR* images. A single observer, blinded to clinical data and GBCA use, reviewed marked WMLs on FLAIR* images for the presence of the CVS. RESULTS. Thirteen of 30 participants had MS. Across participants, on precontrast FLAIR* imaging, 218 CVS-positive and 517 CVS-negative WMLs were identified; on post-contrast FLAIR* imaging, 269 CVS-positive and 459 CVS-negative WMLs were identified. The fraction of WMLs that were CVS-positive on precontrast and postcontrast images was 48% and 58% in participants with MS and 7% and 10% in participants without MS, respectively. The median patient-level CVS-positivity rate on precontrast and postcontrast images was 43% and 67% for participants with MS and 4% and 8% for participants without MS, respectively. In a binomial model adjusting for MS diagnoses, GBCA use was associated with an increased likelihood of at least one CVS-positive WML (odds ratio, 1.6; p < .001). At a 40% CVS-positivity threshold, the sensitivity of the CVS for MS increased from 62% on precontrast images to 92% on postcontrast images (p = .046). Specificity was not significantly different between precontrast (88%) and postcontrast (82%) images (p = .32). CONCLUSION. GBCA use increased CVS detection on FLAIR* images, thereby increasing the sensitivity of the CVS for MS diagnoses. CLINICAL IMPACT. The postcontrast FLAIR* sequence should be considered for CVS evaluation in future investigational trials and clinical practice.
Keywords: FLAIR*; central vein sign; gadolinium; multiple sclerosis.
Figures
Comment in
-
Editorial Comment: Gadolinium-Based Contrast Agent and the Central Vein Sign.AJR Am J Roentgenol. 2023 Jan;220(1):125. doi: 10.2214/AJR.22.28454. Epub 2022 Sep 7. AJR Am J Roentgenol. 2023. PMID: 36069490 No abstract available.
References
-
- Kavaliunas A, Manouchehrinia A, Stawiarz L, et al. Importance of early treatment initiation in the clinical course of multiple sclerosis. Mult Scler 2017; 23:1233–1240 - PubMed
-
- Kaisey M, Solomon AJ, Luu M, Giesser BS, Sicotte NL. Incidence of multiple sclerosis misdiagnosis in referrals to two academic centers. Mult Scler Relat Disord 2019; 30:51–56 - PubMed
-
- Sati P, Oh J, Constable RT, et al.; NAIMS Cooperative. The central vein sign and its clinical evaluation for the diagnosis of multiple sclerosis: a consensus statement from the North American Imaging in Multiple Sclerosis Cooperative. Nat Rev Neurol 2016; 12:714–722 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
