

Do Community-level Disadvantages Account for Racial Disparities in the Safety of Spine Surgery? A Large Database Study Based on Medicare Claims
- PMID: 35976183
- PMCID: PMC9831153
- DOI: 10.1097/CORR.0000000000002323
Do Community-level Disadvantages Account for Racial Disparities in the Safety of Spine Surgery? A Large Database Study Based on Medicare Claims
Abstract
Background: Racial health disparities across orthopaedic surgery subspecialties, including spine surgery, are well established. However, the underlying causes of these disparities, particularly relating to social determinants of health, are not fully understood.
Questions/purposes: (1) Is there a racial difference in 90-day mortality, readmission, and complication rates ("safety outcomes") among Medicare beneficiaries after spine surgery? (2) To what degree does the Centers for Disease Control and Prevention Social Vulnerability Index (SVI), a community-level marker of social determinants of health, account for racial disparities in safety outcomes?
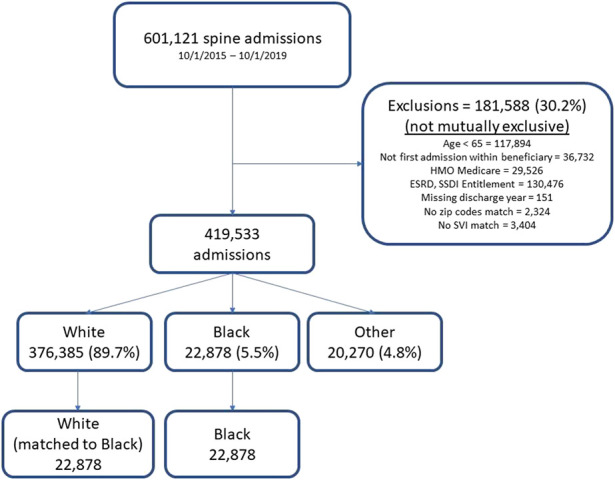
Methods: To examine racial differences in 90-day mortality, readmission, and complications after spine surgery, we retrospectively identified all 419,533 Medicare beneficiaries aged 65 or older who underwent inpatient spine surgery from 2015 to 2019; we excluded 181,588 patients with endstage renal disease or Social Security disability insurance entitlements, who were on Medicare HMO, or who had missing SVI data. Because of the nearly universal coverage of those age 65 or older, Medicare data offer a large cohort that is broadly generalizable, provides improved precision for relatively rare safety outcomes, and is free of confounding from differential insurance access across races. The Master Beneficiary Summary File includes enrollees' self-reported race based on a restrictive list of mutually exclusive options. Even though this does not fully capture the entirety of racial diversity, it is self-reported by patients. Identification of spine surgery was based on five Diagnosis Related Groups labeled "cervical fusion," "fusion, except cervical," "anterior-posterior combined fusion," "complex fusion," and "back or neck, except fusion." Although heterogeneous, these cohorts do not reflect inherently different biology that would lead us to expect differences in safety outcomes by race. We report specific types of complications that did and did not involve readmission. Although complications vary in severity, we report them as composite measures while being cognizant of the inherent limitations of making inferences based on aggregate measures. The SVI was chosen as the mediating variable because it aggregates important social determinants of health and has been shown to be a marker of high risk of poor public health response to external stressors. Patients were categorized into three groups based on a ranking of the four SVI themes: socioeconomic status, household composition, minority status and language, and housing and transportation. We report the "average race effects" among Black patients compared with White patients using nearest-neighbor Mahalanobis matching by age, gender, comorbidities, and spine surgery type. Mahalanobis matching provided the best balance among propensity-type matching methods. Before matching, Black patients in Medicare undergoing spine surgery were disproportionately younger with more comorbidities and were less likely to undergo cervical fusion. To estimate the contribution of the SVI on racial disparities in safety outcomes, we report the average race effect between models with and without the addition of the four SVI themes.
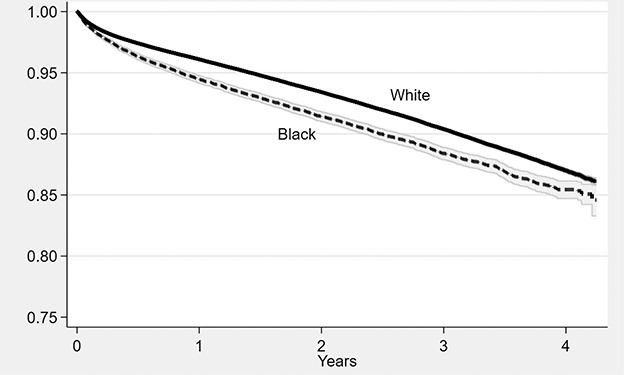
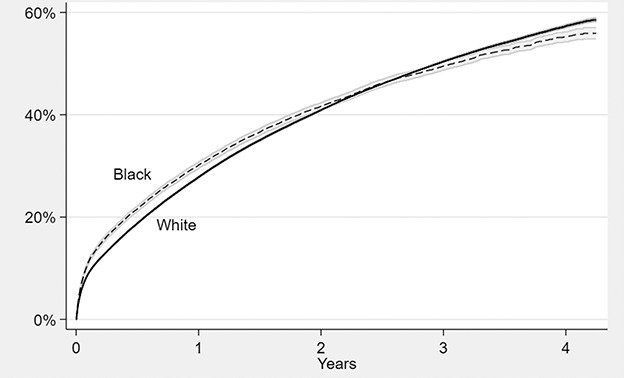
Results: After matching on age, gender, comorbidities, and spine surgery type, Black patients were on average more likely than White patients to be readmitted (difference of 1.5% [95% CI 0.9% to 2.1%]; p < 0.001) and have complications with (difference of 1.2% [95% CI 0.5% to 1.9%]; p = 0.002) or without readmission (difference of 3.6% [95% CI 2.9% to 4.3%]; p < 0.001). Adding the SVI to the model attenuated these differences, explaining 17% to 49% of the racial differences in safety, depending on the outcome. An observed higher rate of 90-day mortality among Black patients was explained entirely by matching using non-SVI patient demographics (difference of 0.00% [95% CI -0.3% to 0.3%]; p = 0.99). However, even after adjusting for the SVI, Black patients had more readmissions and complications.
Conclusion: Social disadvantage explains up to nearly 50% of the disparities in safety outcomes between Black and White Medicare patients after spine surgery. This argument highlights an important contribution of socioeconomic circumstances and societal barriers to achieving equal outcomes. But even after accounting for the SVI, there remained persistently unequal safety outcomes among Black patients compared with White patients, suggesting that other unmeasured factors contribute to the disparities. This is consistent with evidence documenting Black patients' disadvantages within a system of seemingly equal access and resources. Research on racial health disparities in orthopaedics should account for the SVI to avoid suggesting that race causes any observed differences in complications among patients when other factors related to social deprivation are more likely to be determinative. Focused social policies aiming to rectify structural disadvantages faced by disadvantaged communities may lead to a meaningful reduction in racial health disparities.
Level of evidence: Level III, therapeutic study.
Copyright © 2022 by the Association of Bone and Joint Surgeons.
Conflict of interest statement
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research® editors and board members are on file with the publication and can be viewed on request.
Figures
Comment in
-
CORR Insights®: Do Community-level Disadvantages Account for Racial Disparities in the Safety of Spine Surgery? A Large Database Study Based on Medicare Claims.Clin Orthop Relat Res. 2023 Feb 1;481(2):279-280. doi: 10.1097/CORR.0000000000002417. Epub 2022 Sep 20. Clin Orthop Relat Res. 2023. PMID: 36125493 Free PMC article. No abstract available.
References
-
- Abadie A, Imbens GW. Large sample properties of matching estimators for average treatment effects. Econometrica. 2006;74:235-267.
-
- Adler NE, Newman K. Socioeconomic disparities in health: pathways and policies. Health Aff (Millwood). 2002;21:60-76. - PubMed
-
- Adogwa O, Elsamadicy AA, Mehta AI, et al. Racial disparities in 30-day readmission rates after elective spine surgery: a single institutional experience. Spine (Phila Pa 1976). 2016;41:1677-1682. - PubMed
-
- Aladdin DEH, Tangel V, Lui B, et al. Black race as a social determinant of health and outcomes after lumbar spinal fusion surgery: a multistate analysis, 2007 to 2014. Spine (Phila Pa 1976). 2020;45:701-711. - PubMed
-
- Amen TB, Varady NH, Rajaee S, et al. Persistent racial disparities in utilization rates and perioperative metrics in total joint arthroplasty in the U.S.: a comprehensive analysis of trends from 2006 to 2015. J Bone Joint Surg Am. 2020;102:811-820. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
