

Reducing pelvic floor injury by induction of labor
- PMID: 35976420
- PMCID: PMC9383672
- DOI: 10.1007/s00192-022-05296-1
Reducing pelvic floor injury by induction of labor
Abstract
Introduction and hypothesis: We hypothesized that elective induction of labor (eIOL) at 39 weeks is protective of levator ani muscle injury (LAMI) and is associated with decreased pelvic symptoms at 6 weeks postpartum compared to expectant management of labor.
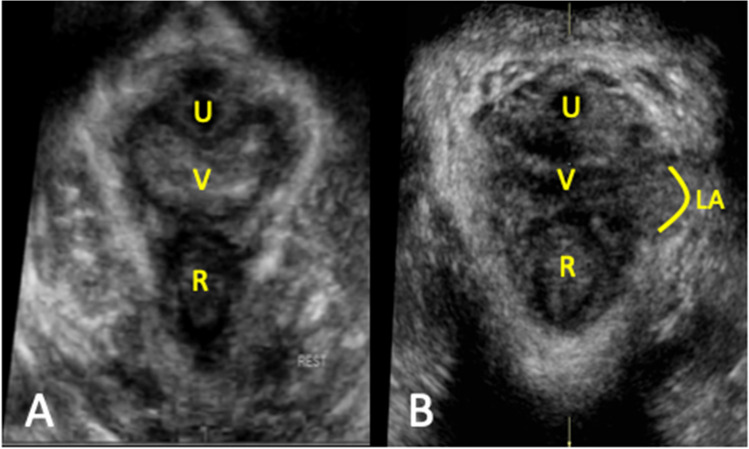
Methods: Prospective cohort pilot study of uncomplicated, primiparous women with a singleton, vertex gestation enrolled immediately post-vaginal delivery (VD). Subjects were dichotomized into two groups based on labor management: eIOL without complication defined by the ARRIVE trial versus spontaneous VD between 39 weeks0/7 and 42 weeks5/7 or no indication for IOL prior to 40 weeks5/7. The primary outcome was LAMI at 6 weeks postpartum as evidenced by any of the following ultrasound measures: (1) increased levator hiatal area (LHA) > 2500 mm2, (2) increased elasticity index (EI, > 75th quartile) or (3) levator enthesis avulsion.
Results: Analysis represents 45/102 consented women from July 2019-October 2020 (eIOL n = 22 and spontaneous VD, n = 23). Neither maternal, clinical, sociodemographic characteristics nor pelvic symptoms differed between groups. Fewer women had LAMI as defined by the primary outcome with eIOL (n = 5, 23.8%) compared to spontaneous VD (n = 15, 65.2%), p = 0.008. Levator enthesis was more deformable (increased EI) with spontaneous VD as compared to the eIOL [10.66 (8.99) vs. 5.68 (2.93), p = 0.046]. On univariate logistic regression women undergoing spontaneous VD had unadjusted OR of 6.0 (1.6-22.5, p = 0.008) of sustaining LAMI compared to those undergoing eIOL.
Conclusions: Composite measures of LAMI though not pelvic floor symptoms were markedly increased in women undergoing spontaneous VD compared to those undergoing eIOL at 39 weeks.
Keywords: Birth injury; Elastography; Elective induction; Obstetric injury; Pelvic floor disorder; Transperineal ultrasound.
© 2022. The International Urogynecological Association.
Conflict of interest statement
None.
Figures


References
-
- Subak LL, Waetjen LE, Van Den Eeden S, Thom DH, Vittinghoff E, Brown JS. Cost of pelvic organ prolapse surgery in the United States. Obstet Gynecol. 2001;98(4):646–51. - PubMed
-
- Wilson L, Brown JS, Shind GP, Luca KO, Subak LL. Annual direct cost of urinary incontinence. Obstet Gynecol. 2001;98(3):398–406. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
