

Comorbidities complicating heart failure: changes over the last 15 years
- PMID: 35976430
- PMCID: PMC9849176
- DOI: 10.1007/s00392-022-02076-1
Comorbidities complicating heart failure: changes over the last 15 years
Abstract
Aims: Management of comorbidities represents a critical step in optimal treatment of heart failure (HF) patients. However, minimal attention has been paid whether comorbidity burden and their prognostic value changes over time. Therefore, we examined the association between comorbidities and clinical outcomes in HF patients between 2002 and 2017.
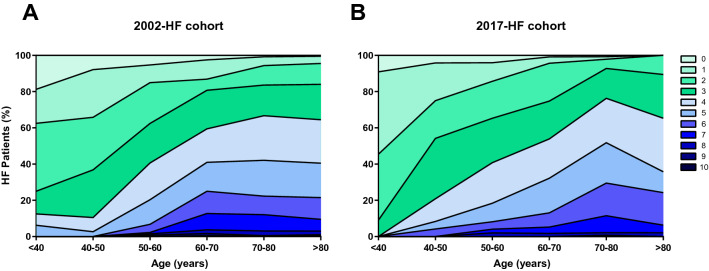
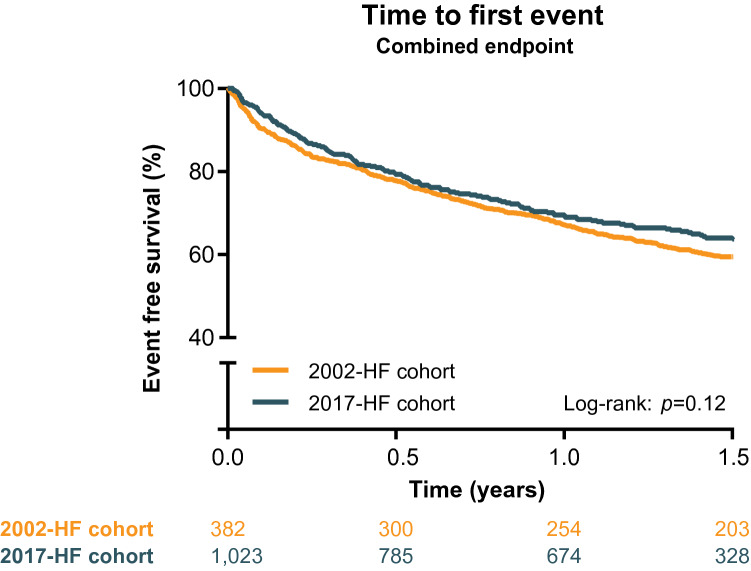
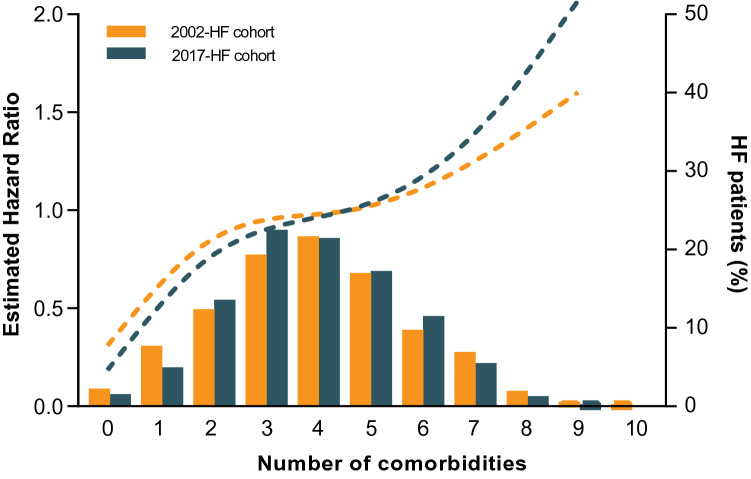
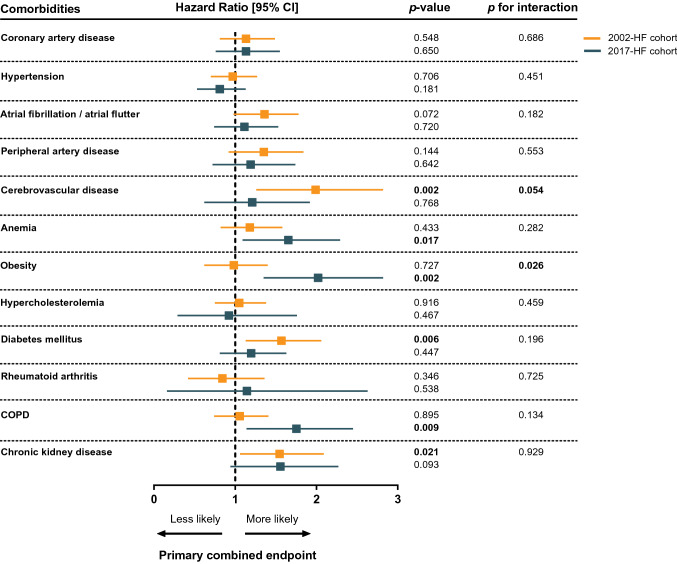
Methods and results: The 2002-HF cohort consisted of patients from The Coordinating Study Evaluating Outcomes of Advising and Counseling in Heart Failure (COACH) trial (n = 1,032). The 2017-HF cohort were outpatient HF patients enrolled after hospitalization for HF in a tertiary referral academic hospital (n = 382). Kaplan meier and cox regression analyses were used to assess the association of comorbidities with HF hospitalization and all-cause mortality. Patients from the 2017-cohort were more likely to be classified as HF with preserved ejection fraction (24 vs 15%, p < 0.001), compared to patients from the 2002-cohort. Comorbidity burden was comparable between both cohorts (mean of 3.9 comorbidities per patient) and substantially increased with age. Higher comorbidity burden was significantly associated with a comparable increased risk for HF hospitalization and all-cause mortality (HR 1.12 [1.02-1.22] and HR 1.18 [1.05-1.32]), in the 2002- and 2017-cohort respectively. When assessing individual comorbidities, obesity yielded a statistically higher prognostic effect on outcome in the 2017-cohort compared to the 2002-HF cohort (p for interaction 0.026).
Conclusion: Despite major advances in HF treatment over the past decades, comorbidity burden remains high in HF and influences outcome to a large extent. Obesity emerges as a prominent comorbidity, and efforts should be made for prevention and treatment. Created with BioRender.com.
Keywords: Comorbidities; Heart failure; Hospitalization; Mortality; Obesity.
© 2022. The Author(s).
Conflict of interest statement
The UMCG, which employs several of the authors has received research grants and/or fees from AstraZeneca, Abbott, Boehringer Ingelheim, Cardior Pharmaceuticals Gmbh, Ionis Pharmaceuticals, Inc., Novo Nordisk, and Roche. Dr. de Boer received speaker fees from Abbott, AstraZeneca, Bayer, Novartis, and Roche. All other authors report no disclosures.
Figures
References
-
- Braunstein JB, Anderson GF, Gerstenblith G, Weller W, Niefeld M, Herbert R, et al. Noncardiac comorbidity increases preventable hospitalizations and mortality among medicare beneficiaries with chronic heart failure. J Am Coll Cardiol. 2003;42:1226–1233. doi: 10.1016/s0735-1097(03)00947-1. - DOI - PubMed
-
- Steinberg BA, Zhao X, Heidenreich PA, Peterson ED, Bhatt DL, Cannon CP, et al. Trends in patients hospitalized with heart failure and preserved left ventricular ejection fraction: Prevalence, therapies, and outcomes. Circulation. 2012;126:65–75. doi: 10.1161/CIRCULATIONAHA.111.080770. - DOI - PubMed
MeSH terms
Grants and funding
- CVON SHE-PREDICTS-HF/Hartstichting
- grant 2017-21/Hartstichting
- CVON RED-CVD/Hartstichting
- grant 2017-11/Hartstichting
- CVON PREDICT2/Hartstichting
- grant 2018-30/Hartstichting
- CVON DOUBLE DOSE/Hartstichting
- grant 2020B005/Hartstichting
- grant 2000Z003/Hartstichting
- Dekker grant 03-005-2021-T005/Hartstichting
- Cure PhosphoLambaN induced Cardiomyopathy (Cure-PLaN)/Fondation Leducq
- ERC CoG 818715/H2020 European Research Council
- SECRETE-HF/H2020 European Research Council
- Mandema-Stipendium of the Junior Scientific Masterclass 2020-10/Universitair Medisch Centrum Groningen
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
