

SOCS1 Haploinsufficiency Presenting as Severe Enthesitis, Bone Marrow Hypocellularity, and Refractory Thrombocytopenia in a Pediatric Patient with Subsequent Response to JAK Inhibition
- PMID: 35976468
- PMCID: PMC9381392
- DOI: 10.1007/s10875-022-01346-x
SOCS1 Haploinsufficiency Presenting as Severe Enthesitis, Bone Marrow Hypocellularity, and Refractory Thrombocytopenia in a Pediatric Patient with Subsequent Response to JAK Inhibition
Abstract
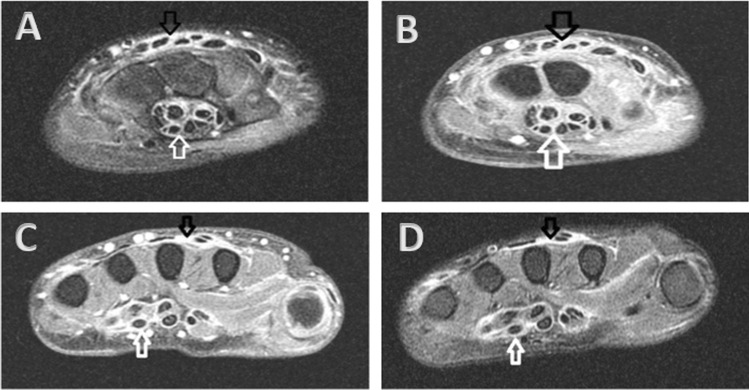
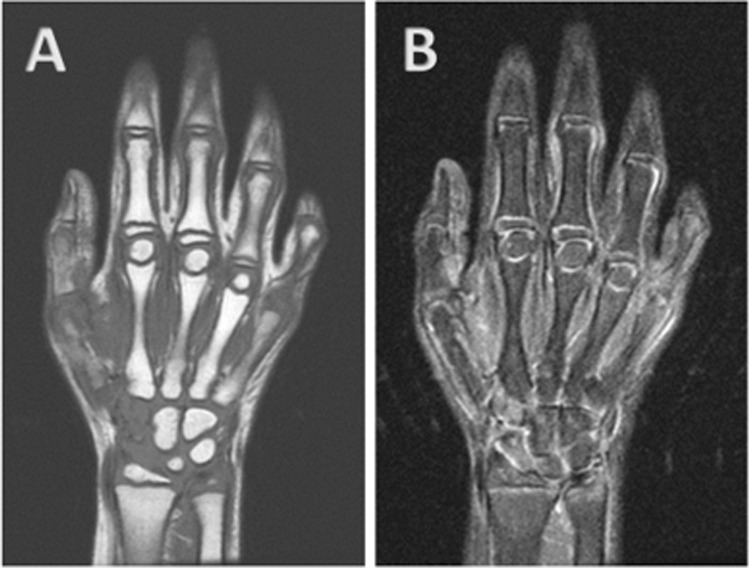
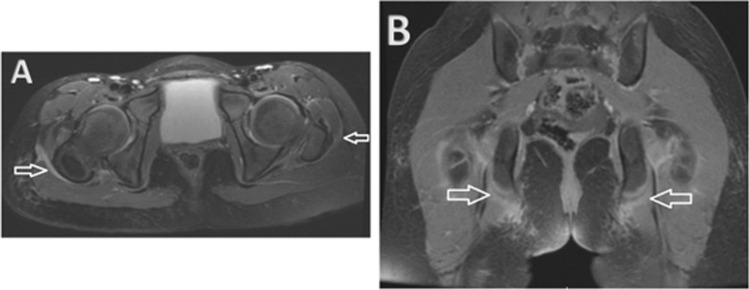
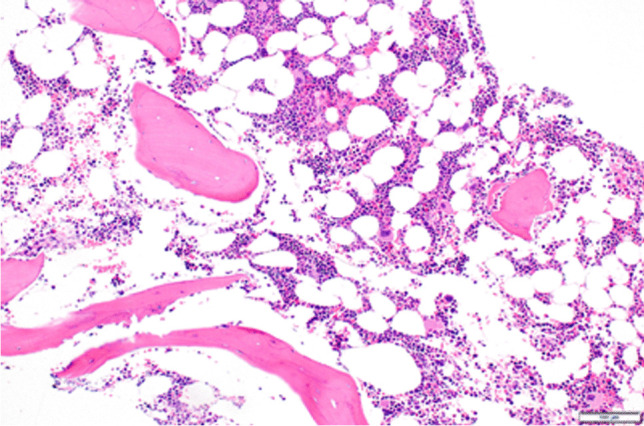
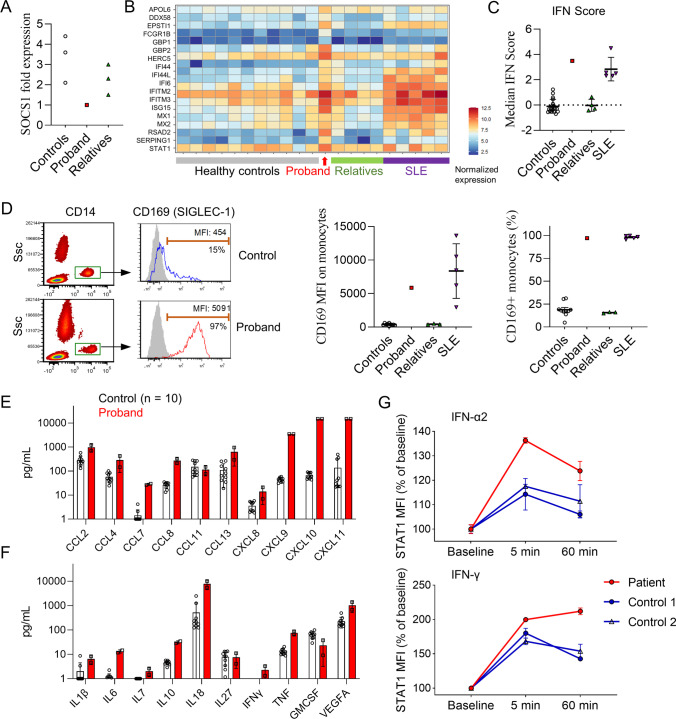
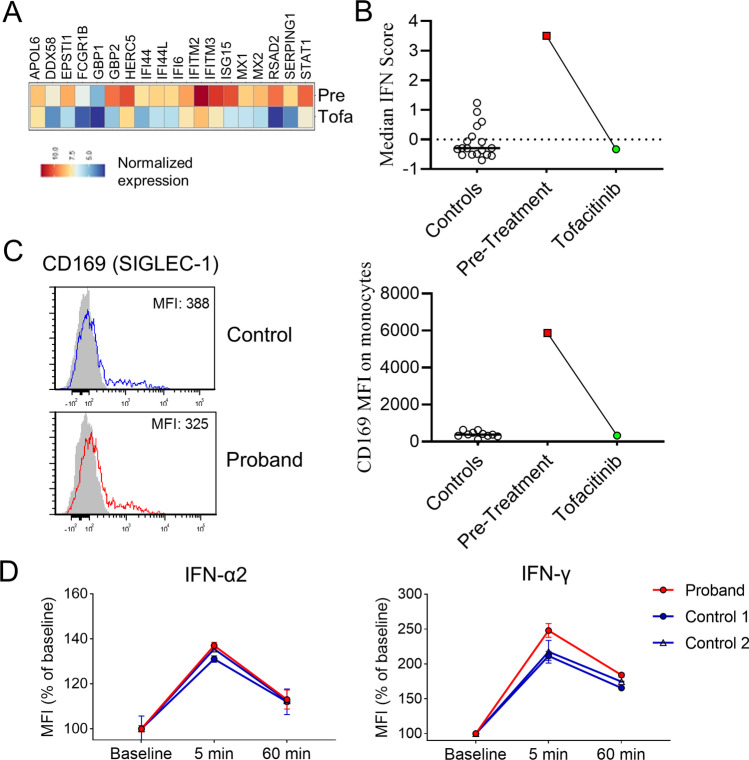
Haploinsufficiency of suppressor of cytokine signaling 1 (SOCS1) is a recently discovered autoinflammatory disorder with significant rheumatologic, immunologic, and hematologic manifestations. Here we report a case of SOCS1 haploinsufficiency in a 5-year-old child with profound arthralgias and immune-mediated thrombocytopenia unmasked by SARS-CoV-2 infection. Her clinical manifestations were accompanied by excessive B cell activity, eosinophilia, and elevated IgE levels. Uniquely, this is the first report of SOCS1 haploinsufficiency in the setting of a chromosomal deletion resulting in complete loss of a single SOCS1 gene with additional clinical findings of bone marrow hypocellularity and radiologic evidence of severe enthesitis. Immunologic profiling showed a prominent interferon signature in the patient's peripheral blood mononuclear cells, which were also hypersensitive to stimulation by type I and type II interferons. The patient showed excellent clinical and functional laboratory response to tofacitinib, a Janus kinase inhibitor that disrupts interferon signaling. Our case highlights the need to utilize a multidisciplinary diagnostic approach and consider a comprehensive genetic evaluation for inborn errors of immunity in patients with an atypical immune-mediated thrombocytopenia phenotype.
Keywords: Autoinflammatory syndrome; Bone marrow hypocellularity; Immune thrombocytopenia; Interferonopathy; JAK inhibition; SOCS1 haploinsufficiency.
© 2022. The Author(s), under exclusive licence to Springer Science+Business Media, LLC, part of Springer Nature.
Conflict of interest statement
No authors have competing interests. Michniacki, Saad, Hannibal, DeMeyer, Brown, Mohan, Lee, Ngo, Simoneau, Chen, Brodeur, Du, Basiaga, Horst: No disclosures. Frame: Research Funding from Jazz Pharmaceuticals. Walkovich: Horizon Pharmaceuticals: Honoraria, Membership on an entity’s Board of Directors or advisory committees; Pharming: Honoraria, Membership on an entity’s Board of Directors or advisory committees; Swedish Orphan Biovitrum AB (Sobi): Consultancy, Honoraria; X4 Pharmaceuticals: Other: Local PI for clinical trial involving mavorixafor and patients with neutropenia.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
