

Antihypertensive Effect of Long-Term Monotherapy with Esaxerenone in Patients with Essential Hypertension: Relationship Between Baseline Urinary Sodium Excretion and Its Antihypertensive Effect
- PMID: 35976603
- PMCID: PMC9464726
- DOI: 10.1007/s12325-022-02282-3
Antihypertensive Effect of Long-Term Monotherapy with Esaxerenone in Patients with Essential Hypertension: Relationship Between Baseline Urinary Sodium Excretion and Its Antihypertensive Effect
Abstract
Introduction: The blood pressure (BP) control mechanism for mineralocorticoid receptor blockers is unclear, and analysis of their use as a single agent in the clinical setting is required to resolve this uncertainty. There is a paucity of data on esaxerenone monotherapy assessing its long-term antihypertensive effect and urinary biomarkers.
Methods: This post hoc exploratory substudy of a long-term phase 3 study evaluated the effect of esaxerenone monotherapy (2.5 or 5 mg/day) in treatment-naïve patients who continued the therapy during the 52-week study period (n = 25). In addition to blood biomarkers, urinary biomarkers were also assessed in 24-h urine collection samples.
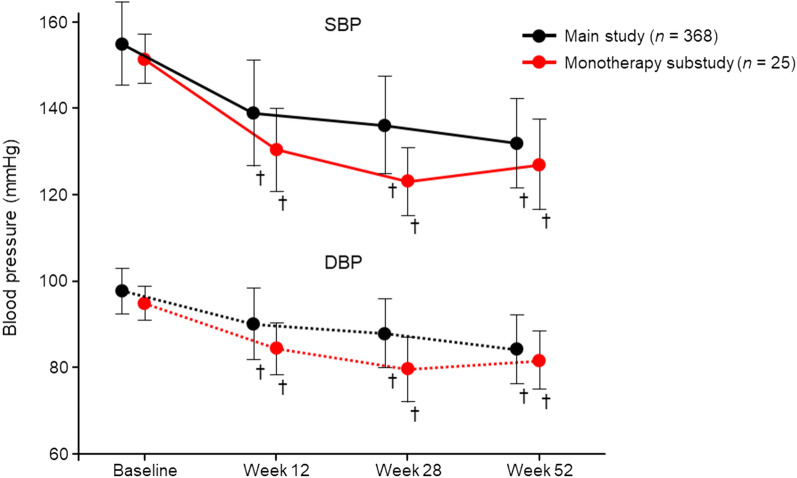
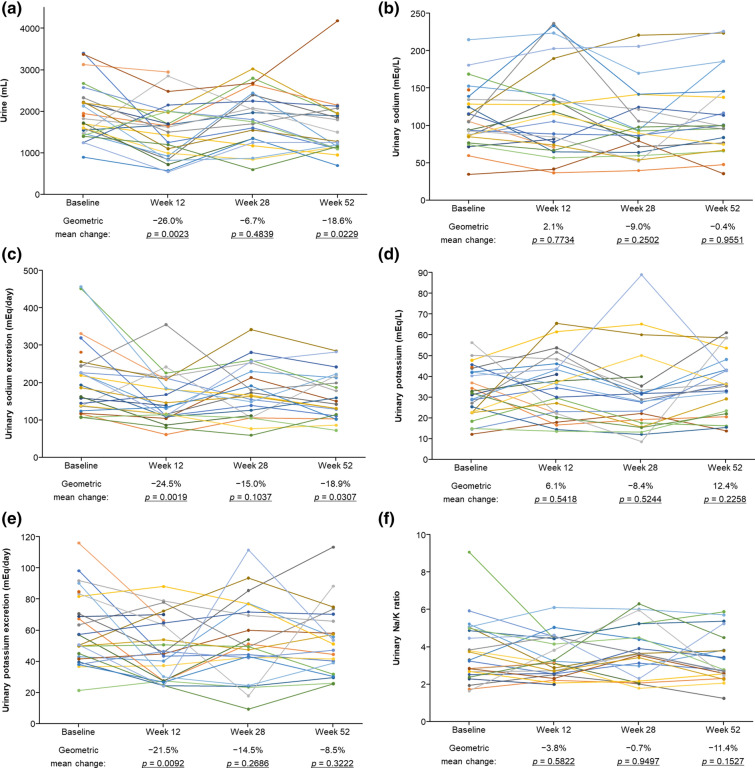
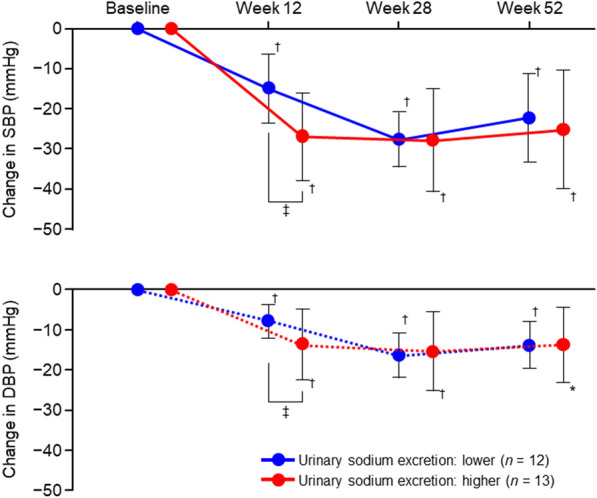
Results: Esaxerenone monotherapy was associated with consistent reductions in systolic/diastolic BP in the substudy population (- 23.5/- 13.1 mmHg at week 52, p < 0.001 vs baseline). Plasma aldosterone concentrations and plasma renin activity significantly increased during esaxerenone monotherapy at all time points. On the basis of the observations that both urine volume and urinary sodium excretion also decreased up to the end of the study, and were significantly lower at 12 weeks, patients were further categorized into higher/lower urinary sodium excretion subgroups according to whether their baseline values were above or below the median. In the group with higher baseline urinary sodium excretion, esaxerenone exhibited a significantly greater decrease in systolic/diastolic BP compared to the lower baseline group.
Conclusion: Esaxerenone exhibited sustained and stable antihypertensive activity even when administered as a single agent for 52 weeks in patients with essential hypertension. The additional urinary biomarker analysis suggests that the BP-lowering effects of esaxerenone may be partly exerted via mechanisms related to salt and water retention, and that the effect is particularly pronounced in patients with hypertension and higher baseline urinary sodium excretion, which may reflect a state of excessive salt intake.
Trial registration: NCT02722265.
Keywords: Esaxerenone; Excessive salt intake; Long-term monotherapy; Mineralocorticoid receptor blocker; Urinary sodium excretion.
© 2022. The Author(s).
Figures
References
-
- Esteras R, Perez-Gomez MV, Rodriguez-Osorio L, Ortiz A, Fernandez-Fernandez B. Combination use of medicines from two classes of renin-angiotensin system blocking agents: risk of hyperkalemia, hypotension, and impaired renal function. Ther Adv Drug Saf. 2015;6:166–176. doi: 10.1177/2042098615589905. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
