

Addition of FFRct in the diagnostic pathway of patients with stable chest pain to reduce unnecessary invasive coronary angiography (FUSION) : Rationale and design for the multicentre, randomised, controlled FUSION trial
- PMID: 35976610
- PMCID: PMC9892409
- DOI: 10.1007/s12471-022-01711-w
Addition of FFRct in the diagnostic pathway of patients with stable chest pain to reduce unnecessary invasive coronary angiography (FUSION) : Rationale and design for the multicentre, randomised, controlled FUSION trial
Abstract
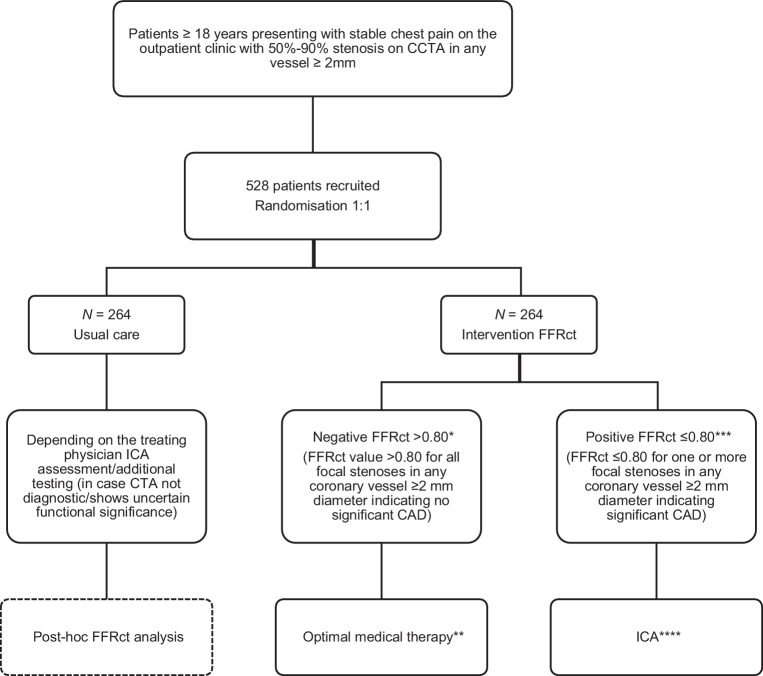
Background: Coronary computed tomography angiography (CCTA) is widely used in the diagnostic work-up of patients with stable chest pain. CCTA has an excellent negative predictive value, but a moderate positive predictive value for detecting coronary stenosis. Computed tomography-derived fractional flow reserve (FFRct) is a non-invasive, well-validated technique that provides functional assessment of coronary stenosis, improving the positive predictive value of CCTA. However, to determine the value of FFRct in routine clinical practice, a pragmatic randomised, controlled trial (RCT) is required. We will conduct an RCT to investigate the impact of adding FFRct analysis in the diagnostic pathway of patients with a coronary stenosis on CCTA on the rate of unnecessary invasive coronary angiography, cost-effectiveness, quality of life and clinical outcome.
Methods: The FUSION trial is a prospective, multicentre RCT that will randomise 528 patients with stable chest pain and anatomical stenosis of ≥ 50% but < 90% in at least one coronary artery of ≥ 2 mm on CCTA, to FFRct-guided care or usual care in a 1:1 ratio. Follow-up will be 1 year. The primary endpoint is the rate of unnecessary invasive coronary angiography within 90 days.
Conclusion: The FUSION trial will evaluate the use of FFRct in stable chest pain patients from the Dutch perspective. The trial is funded by the Dutch National Health Care Institute as part of the research programme 'Potentially Promising Care' and the results will be used to assess if FFRct reimbursement should be included in the standard health care package.
Keywords: Angina; Computed tomography angiography; Coronary angiography; Coronary artery disease; Fractional flow reserve; Myocardial; Stable.
© 2022. The Author(s).
Conflict of interest statement
S.P. Sharma, A. Hirsch, M.G.M. Hunink, M.J.M. Cramer, F.A.A. Mohamed Hoesein, C.A. Geluk, G. Kramer, J.W.C. Gratama, R.L. Braam, P.M. van der Zee, W. Yassi, S.L. Wolters, C. Gürlek, G. Pundziute, R. Vliegenthart and R.P.J. Budde declare that they have no competing interests. This study is financially supported by HeartFlow, Inc. In addition, the Erasmus Medical Centre has received support from HeartFlow, Inc. and Siemens for other studies unrelated to the FUSION trial.
Figures
References
-
- Nederland Z. Verbetersignalement pijn op de borst (verdenking) stabiele angina pectoris. Zorginstituut Nederland; 2017.
-
- NICE . Recent-onset chest pain of suspected cardiac origin: assessment and diagnosis (CG95) 2010. - PubMed
-
- Haase R, Schlattmann P, Gueret P, et al. Diagnosis of obstructive coronary artery disease using computed tomography angiography in patients with stable chest pain depending on clinical probability and in clinically important subgroups: meta-analysis of individual patient data. BMJ. 2019;365:l1945. doi: 10.1136/bmj.l1945. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
