

Analysis of Cancer Survival Associated With Immune Checkpoint Inhibitors After Statistical Adjustment: A Systematic Review and Meta-analyses
- PMID: 35976648
- PMCID: PMC9386543
- DOI: 10.1001/jamanetworkopen.2022.27211
Analysis of Cancer Survival Associated With Immune Checkpoint Inhibitors After Statistical Adjustment: A Systematic Review and Meta-analyses
Abstract
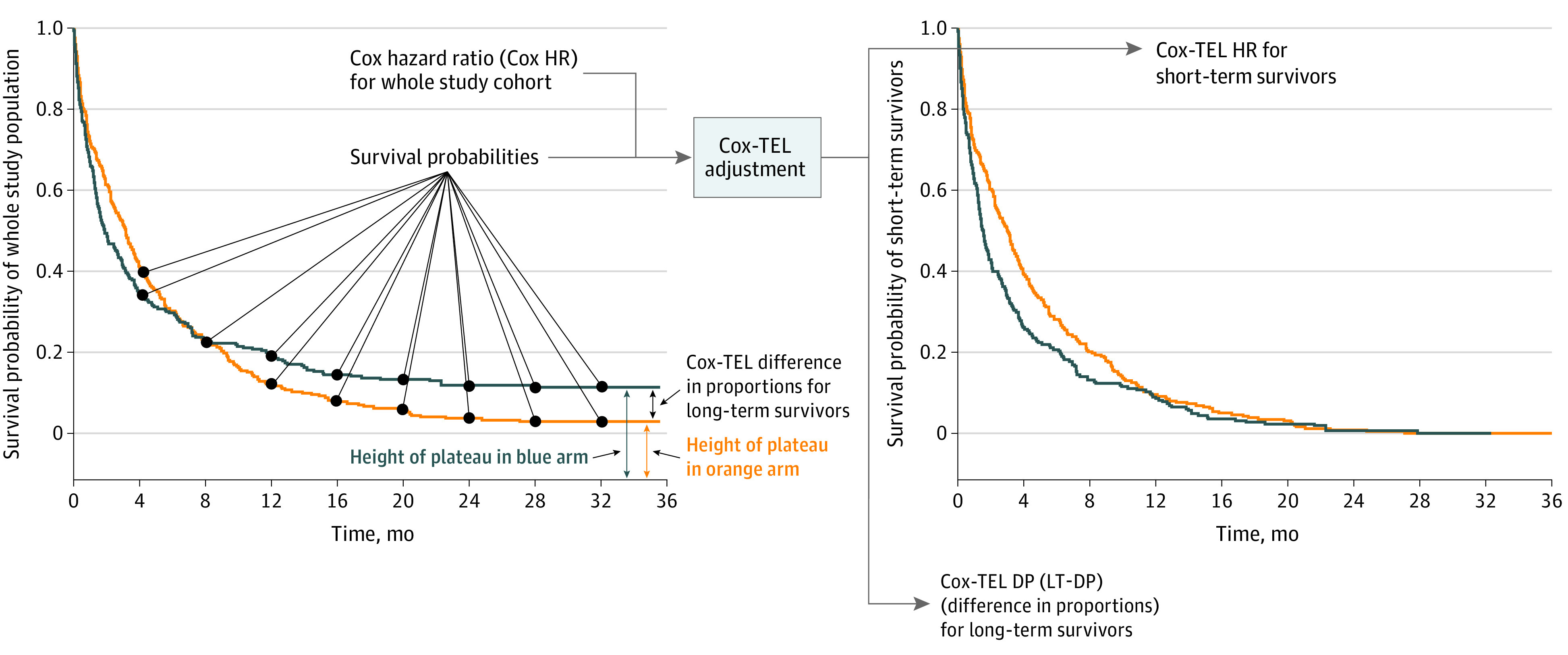
Importance: Appropriate clinical decision-making relies on accurate data interpretation, which in turn relies on the use of suitable statistical models. Long tails and early crossover-2 features commonly observed in immune checkpoint inhibitor (ICI) survival curves-raise questions as to the suitability of Cox proportional hazards regression for ICI survival analysis. Cox proportional hazards-Taylor expansion adjustment for long-term survival data (Cox-TEL) adjustment may provide possible solutions in this setting.
Objective: To estimate overall survival and progression-free survival benefits of ICI therapy vs chemotherapy using Cox-TEL adjustment.
Data sources: A PubMed search was performed for all cataloged publications through May 22, 2022.
Study selection: The search was restricted to randomized clinical trials with search terms for ICIs and lung cancer, melanoma, or urothelial carcinoma. The publications identified were further reviewed for inclusion.
Data extraction and synthesis: Cox proportional hazards ratios (HRs) were transformed to Cox-TEL HRs for patients with short-term treatment response (ie, short-term survivor) (ST-HR) and difference in proportions for patients with long-term survival (LT-DP) by Cox-TEL. Meta-analyses were performed using a frequentist random-effects model.
Main outcomes and measures: Outcomes of interest were pooled overall survival (primary outcome) and progression-free survival (secondary outcome) HRs, ST-HRs, and LT-DPs. Subgroup analyses stratified by cancer type also were performed.
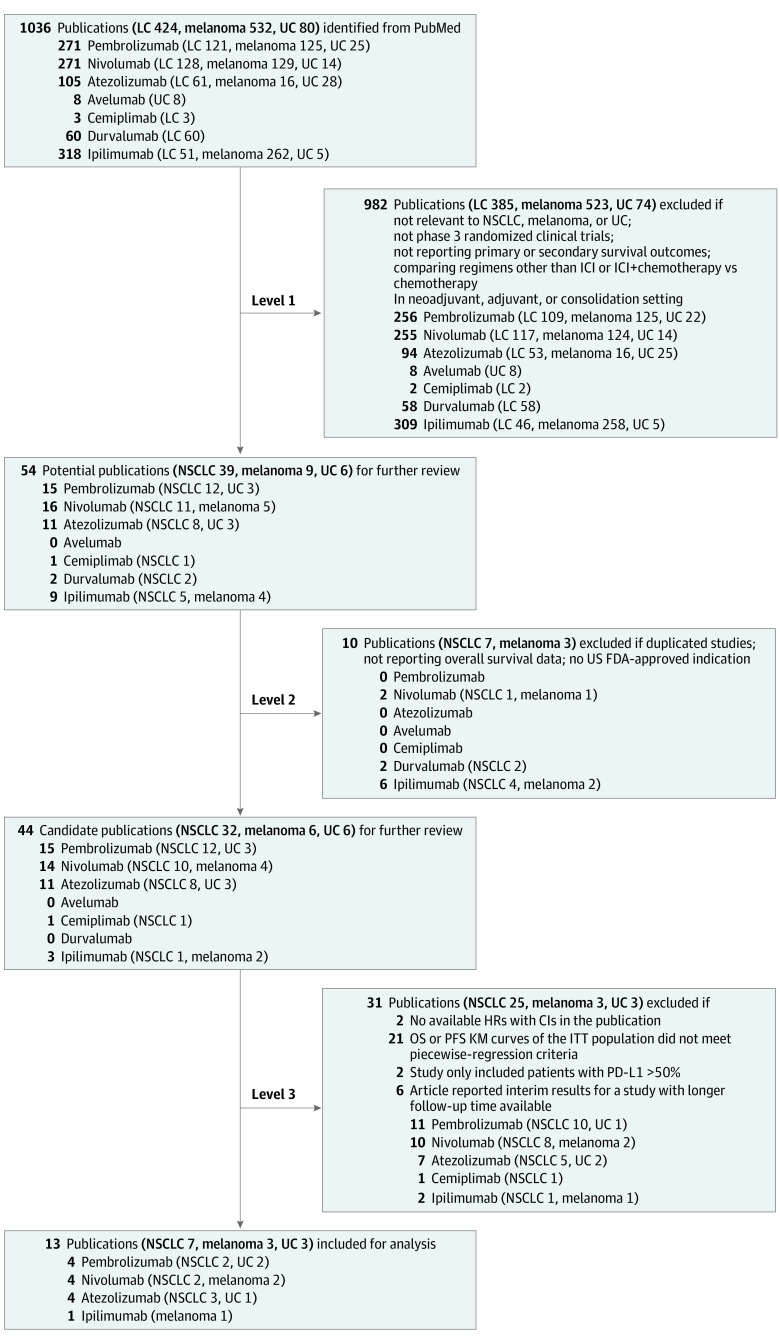
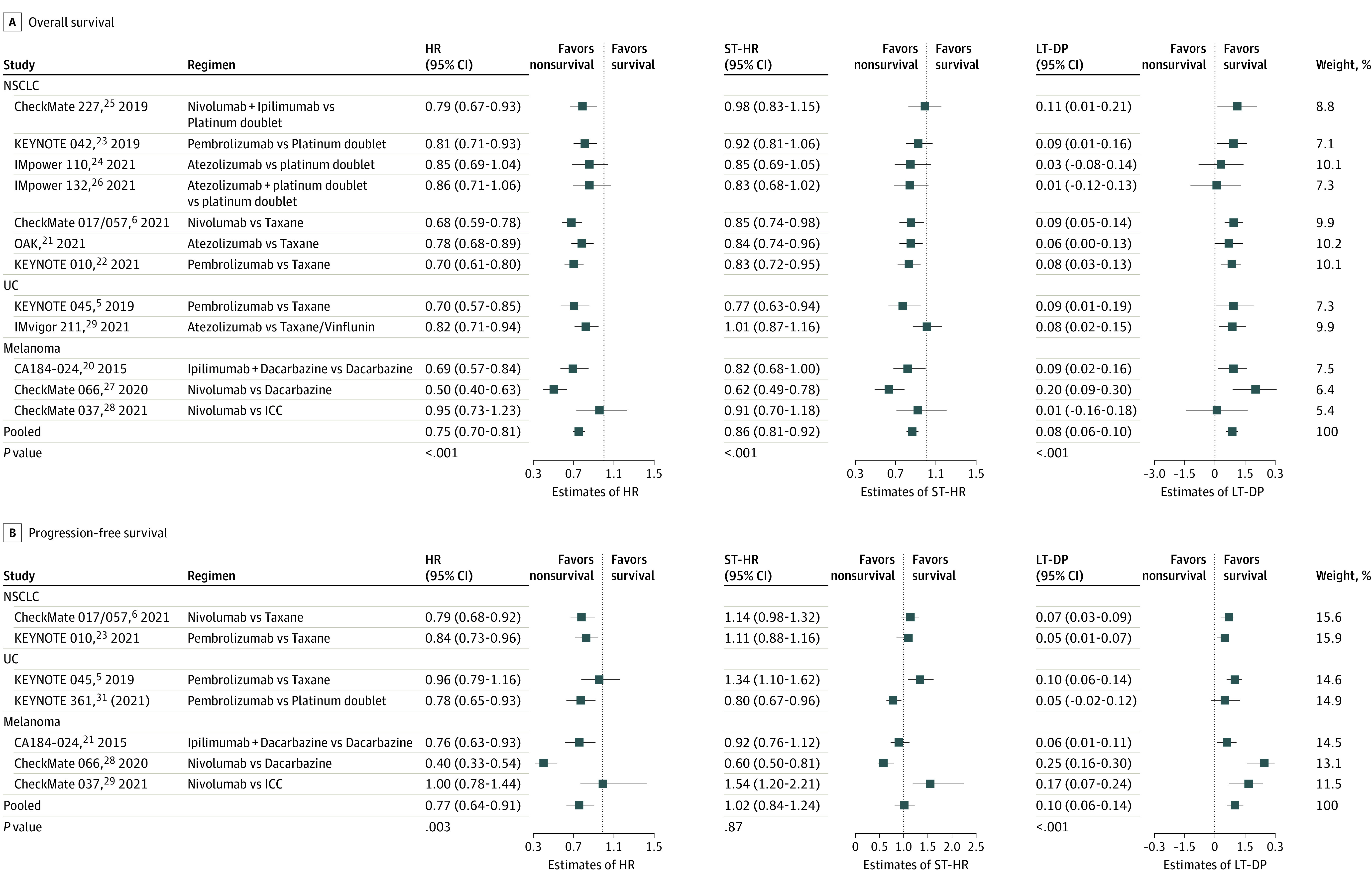
Results: A total of 1036 publications was identified. After 3 levels of review against inclusion criteria, 13 clinical trials (7 in non-small cell lung cancer, 3 in melanoma, and 3 in urothelial carcinoma) were selected for the meta-analysis. In the primary analysis, pooled findings were 0.75 (95% CI, 0.70-0.81) for HR, 0.86 (95% CI, 0.81-0.92) for ST-HR, and 0.08 (95% CI, 0.06-0.10) for LT-DP. In the secondary analysis, the pooled values for progression-free survival were 0.77 (95% CI, 0.64-0.91) for HR, 1.02 (95% CI, 0.84-1.24) for ST-HR, and 0.10 (95% CI, 0.06-0.14) for LT-DP.
Conclusions and relevance: This systematic review and meta-analysis of ICI clinical trial results noted consistently larger ST-HRs vs Cox HRs for ICI therapy, with an LT-DP of approximately 10%. These results suggest that Cox HRs may not provide a full picture of survival outcomes when the risk reduction from treatment is not constant, which may aid in the decision-making process of oncologists and patients.
Conflict of interest statement
Figures
References
-
- Kuk AYC, Chen CH. A mixture model combining logistic regression with proportional hazards regression. Biometrika. 1992;79:531-541. doi: 10.1093/biomet/79.3.531 - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
